1. Stone GW, Christiansen EH, Ali ZA, et al. Intravascular imaging-guided coronary drug-eluting stent implantation: an updated network meta-analysis. Lancet. 2024;403(10429):824-837. doi:10.1016/S0140-6736(23)02454-6
2. Hong S, Mintz G, Ahn C, et al. Effect of Intravascular Ultrasound–Guided Drug-Eluting Stent Implantation. J Am Coll Cardiol Intv. 2020 Jan, 13 (1) 62–71. doi: 10.1016/j.jcin.2019.09.033
3. Gao X, Ge Z, Kong X, et al. 3-Year Outcomes of the ULTIMATE Trial Comparing Intravascular Ultrasound Versus Angiography-Guided Drug-Eluting Stent Implantation. J Am Coll Cardiol Intv. 2021 Feb, 14 (3) 247–257. doi: 10.1016/j.jcin.2020.10.001
4. Lee, JM, Choi, KH, Lee, JY, et. Al. Intravascular Imaging-Guided or Angiography-Guided Complex PCI. N Engl J Med 2023; 388:1668-1679. doi: 10.1056/NEJMoa2216607
5. Li X, Ge Z, Kan J, et al. Intravascular ultrasound-guided versus angiography-guided percutaneous coronary intervention in acute coronary syndromes (IVUS-ACS): a two-stage, multicentre, randomised trial. Lancet. 2024;403(10439):1855-1865. doi:10.1016/S0140-6736(24)00282-4
6. Sung-Jin Hong, MD; Byeong-Keuk Kim, MD; Dong-Ho Shin, MD, MPH; et al. Effect of Intravascular Ultrasound–Guided vs Angiography-Guided Everolimus-Eluting Stent Implantation The IVUS-XPL Randomized Clinical Trial. JAMA. 2015;314(20):2155-2163. doi:10.1001/jama.2015.15454
7. Zhang J, Gao X, Kan J, et al. Intravascular Ultrasound Versus Angiography-Guided Drug-Eluting Stent Implantation: The ULTIMATE Trial. J Am Coll Cardiol Intv. 2018;72(24):3126-3137. doi: 10.1016/j.jacc.2018.09.013
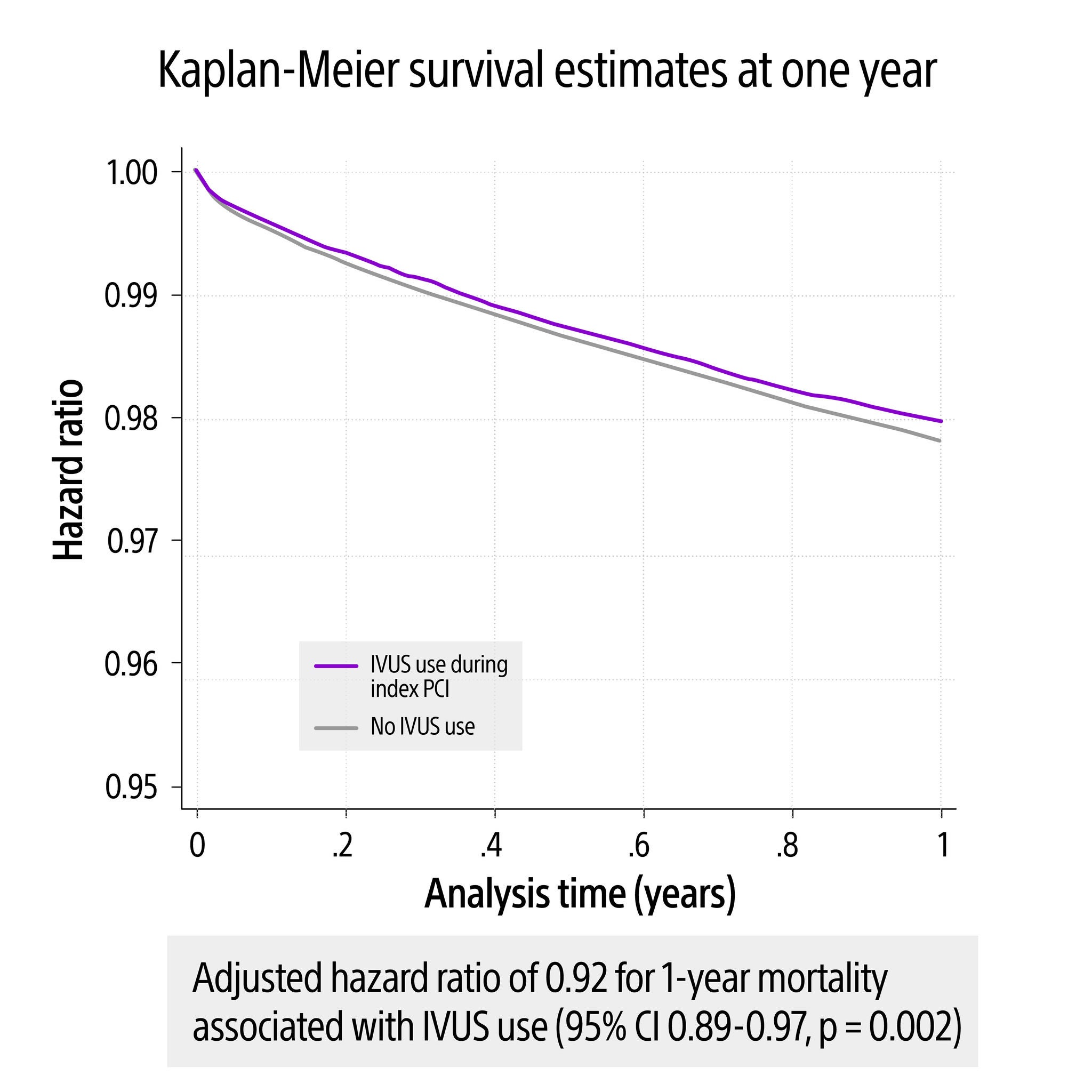
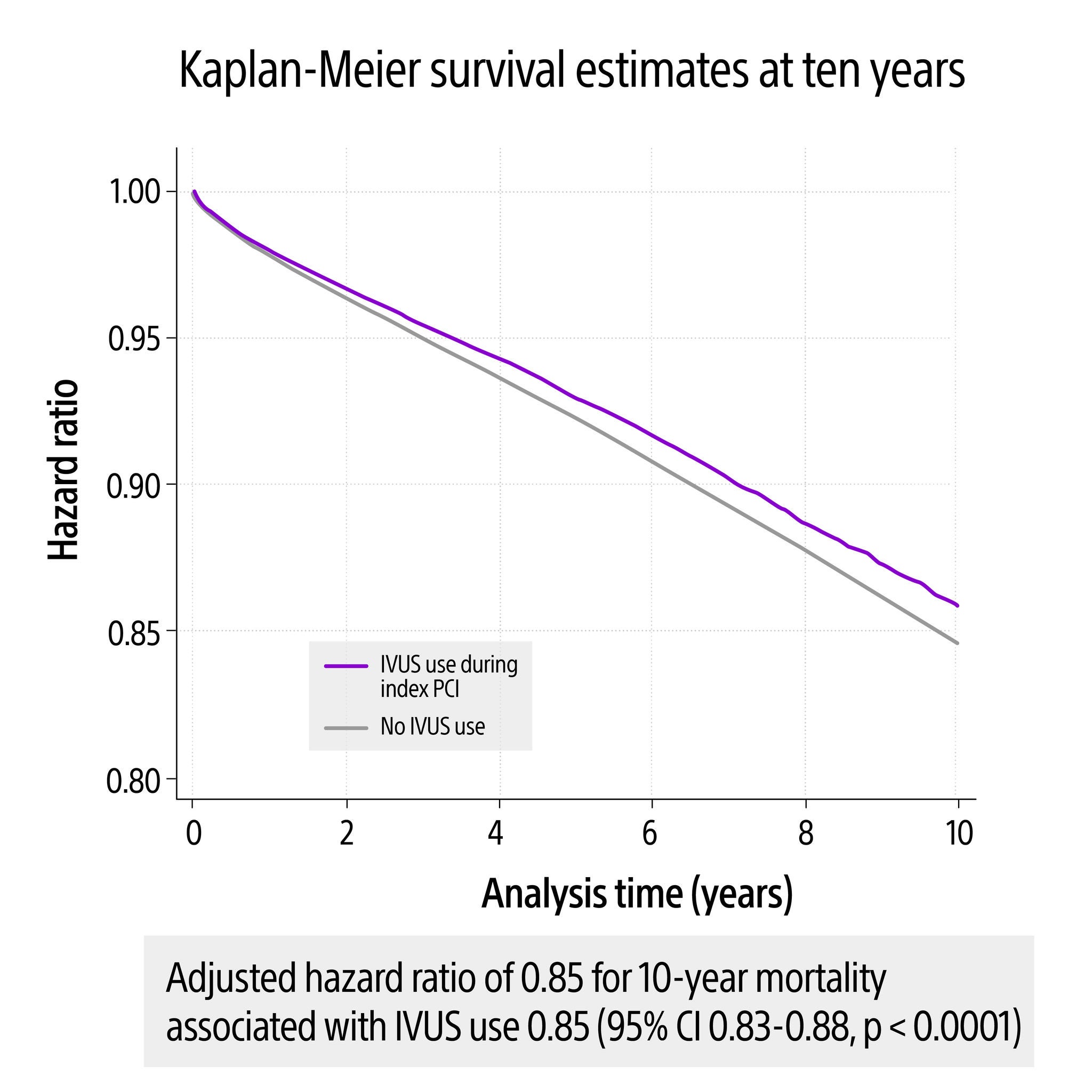
8. Amin, Amit. IVUS use and long-term PCI outcomes in the United States: Insights from the Premier Database. Presented at: CRT 2024. March 9, 2024. Washington, DC, USA.