Boston Scientific accounts are for healthcare professionals only.

Kevin Zorn, M.D.
Department of Urology, University of Montreal Hospital Center CHUM, Montreal, Quebec, Canada
Editorial commentary
Although there are a variety of effective ways to treat moderate to severe benign prostatic hyperplasia (BPH), many of them come with unwanted side effects, require hospitalization, and should be avoided in patients with comorbidities, such as those on anti-coagulants.
The approach I prefer for such cases is the anatomic vaporization incision technique (VIT) using the GreenLight XPS™ Laser Therapy System. The VIT approach is a minimally invasive out-patient procedure that combines the principles of traditional photo-selective vaporization (PVP) and enucleation techniques to identify the surgical capsule early and more completely remove obstructive prostate tissue of the transition zone.1 With greater removal of BPH adenomatous tissue coupled with excellent hemostasis, we are able to provide safe, same-day surgery with rapid restoration of urine flow with reduced post-operative complications.2 The VIT laser approach also allows a systematic, structured and reproducible approach for BPH patients, including those on anticoagulation therapy, with large prostates or with obstructive median lobes.2–7
Although I started out doing BPH surgeries using a holmium laser, I eventually shifted to using the GreenLight Laser, due to its versatility with superior hemostasis and non-contact laser wavelength properties.6,8 Like a Swiss Army knife, GreenLight Therapy offers so many tools in one platform. For example, I use GreenLight Therapy primarily to vaporize tissue, chisel off or enucleate small pieces of tissue, and quickly achieve hemostasis from bleeding vessels.
VIT: The preferred method
The traditional PVP approach vaporizes the unwanted prostate tissue, an approach I often use on smaller prostates, such as those <40–50cc. However, for larger prostates I prefer VIT, which rather than vaporizing the large volume of prostate tissue, essentially strategically cuts out the tissue so it can be removed at the end of the procedure using a grasper or standard TURP loop. In these cases I prefer the VIT technique because it uses less laser energy and reduces the time that it takes to perform the procedure.9 It also allows for tissue samples to be retrieved and examined by a pathologist. The surgical defect is also smoother and has significantly less necrotic tissue compared to traditional PVP10 which, in my experience, results in less dysuria and reduced post-operative clinical visits.
To perform this procedure, I use the GreenLight Therapy XPS LBO-180W system to take advantage of its unique haemostatic 532nm energy wavelength and a wide area of effect. Compared to alternative treatments for large prostates, such as open surgery, this same-day procedure allows patients to avoid hospitalization, heal and recover quickly, minimize complications, and enjoy durable results, all while lowering overall hospital costs.3,5,7,11 There is also no need for the additional morcellation time, equipment, costs, risks and associated complications. More than 90–95% of my patients are discharged home the same day of their procedure.
GreenLight VIT has advantages for elderly patients or those on blood thinners/anticoagulation medications. Since the risk of bleeding complications are significantly reduced, patients do not always need to discontinue their blood thinners before the procedure and have a significantly lower risk of requiring a transfusion.1 As we are most aware, current international guidelines all have consensus to support the use of GreenLight PVP in anti-coagulated men.12,13 The published results are durable, as GreenLight Therapy has been shown to reduce BPH symptoms for up to five years or more.14 We have also demonstrated superior BPH resection with greater improvements in functional outcomes and PSA reduction (63% vs. 50%, p=0.01) at 6 months with VIT in comparison with PVP.10
Laser therapy options
Although there are several alternative laser approaches, including holmium and thulium energy systems with comparable outcomes to VIT, with GreenLight Therapy, there are several reasons I prefer the GreenLight Laser VIT approach.
First, while the energy from holmium or thulium lasers is absorbed by water, GreenLight Laser’s 532nm wavelength is specifically absorbed by hemoglobin.9 As a result, VIT is not impeded by the irrigating agent during the procedure, and can efficiently and rapidly vaporize prostatic tissue.9 In my experience, GreenLight Therapy allows the surgeon to approach the tissue from various angles and distances (up to 3–4mm away from tissue) whereas for holmium and thulium, a direct contact or near contact with tissue is needed to have effect.
Second, there is a lot of mechanical blunt pushing of the adenoma with the holmium laser enucleation of the prostate (HoLEP) procedure which is not needed for GreenLight VIT; as a result, stress incontinence can be a common outcome with HoLEP.15,16 Since VIT does not create the same amount of mechanical torque and tension on the adenoma as does HoLEP, its rates of stress incontinence are much lower.9
My VIT approach
I take a systematic approach with VIT based on proper cystoscopy, knowledge of prostate anatomy with preoperative ultrasound, and routine technique.1 My approach includes:
- Once the size of the prostate is gauged through ultrasound, I use a cystoscope to identify anatomical landmarks, so I can keep myself oriented during the procedure.
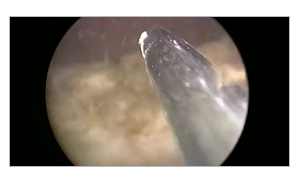
- Next, I vaporize a working space and demarcate the apex adjacent to the verumontanum. (Fig. 1)
 Figure 1: Demarcation of apical limits in front of veru.
Figure 1: Demarcation of apical limits in front of veru.
- Thereafter, I create deepened and widened groves from the bladder neck to the verumontanum at the 5 o’clock and 7 o’clock positions. (Fig. 2)
 Figure 2: Groove creation at 7 o’clock down to capsule.
Figure 2: Groove creation at 7 o’clock down to capsule.
- Then comes the heart of the procedure, in which I systematically debulk the prostate by using the laser to remove the adenoma (non-malignant prostate tissue) off the surgical capsule, pushing tissue pieces that are too large to be vaporized into the bladder. (Fig. 3)
 Figure 3, Part 1: VIT along capsule of floor tissue.
Figure 3, Part 1: VIT along capsule of floor tissue.
 Figure 3, Part 2: VIT along capsule of floor tissue.
Figure 3, Part 2: VIT along capsule of floor tissue.
- This is then repeated for both lateral lobes after a 12 o’clock incision is made through the anterior commissure to the capsule and the lateral adenoma tissue are freed off the capsule. (Fig. 4)
 Figure 4: Incision and release of left sided adenoma.
Figure 4: Incision and release of left sided adenoma.
- Once the debulking is complete, I retrieve the pieces of adenoma tissue from the bladder. (Fig. 5)
- Finally, I examine the area, looking for any pieces of prostate tissue that I have missed and check for bleeding.
 Figure 5: Grasper or loop retrieval of excised adenoma.
Figure 5: Grasper or loop retrieval of excised adenoma.
For those who are interested in a description of this approach, see the article I co-authored in the October 2019 issue of the Canadian Journal of Urology.
Recommendations for surgeons new to VIT
A note for users accustomed to water-based laser techniques: the GreenLight Laser requires a continuous sweeping motion, as opposed to the more static motion of holmium or thulium lasers.1
VIT requires the surgeon to have ample GreenLight Therapy experience. One study shows that it takes 120 PVP procedures for a surgeon to achieve outcomes comparable to experts.17 Surgeons new to VIT are recommended to start with patients who have limited comorbidities and are not on blood thinners, no median lobe, and a small prostate (less than 65 cc).1
Once the surgeon is ready for VIT, it’s important to carefully manage patients by setting realistic expectations. For example, patients should understand that in the first few weeks after the procedure, they may have dysuria, pink urine (debris from the procedure), sperm in their urine (retrograde ejaculation), a urinary tract infection, and/or stress incontinence.1 Patients who understand these possible short-term effects are typically quite calm at their one-month follow-up visit.
Conclusion
By basing VIT on standards, such as proper cystoscopy, knowledge of prostate anatomy with preoperative ultrasound, and routine technique, we can achieve consistent, reproducible, and optimal surgical outcomes. Although there are many treatment alternatives for men with moderate to severe BPH, I believe VIT with the GreenLight System may be our most versatile, safe, effective and durable option.
Related content

References
- Law KW, Elterman DS, Cash H, et al. Anatomic GreenLight laser vaporization-incision technique for benign prostatic hyperplasia using the XPS LBO-180W system: How I do it. Can J Urol. 2019 Oct;26(5):9963–72.
- Bachmann A, Tubaro A, Barber N, et al. A European multicenter randomized noninferiority trial comparing 180 W GreenLight-XPS laser vaporization and transurethral resection of the prostate for the treatment of benign prostatic obstruction: 12-month results of the GOLIATH study. J Urol. 2015 Feb;193(2):570–8.
- Thomas JA, Tubaro A, Barber N, et al. A multicenter randomized noninferiority trial comparing GreenLight-XPS laser vaporization of the prostate and transurethral resection of the prostate for the treatment of benign prostatic obstruction: Two-yr outcomes of the GOLIATH study. Eur Urol. 2016 Jan;69(1):94–102.
- Bachmann A, Tubaro A, Barber N, et al. 180-W XPS GreenLight laser vaporization versus transurethral resection of the prostate for the treatment of benign prostatic obstruction: 6-month safety and efficacy results of a European multicentre randomised trial—the GOLIATH study. Eur Urol. 2014 May;65(5):931–42.
- Goh AC, Gonzalez RR. Photoselective laser vaporization prostatectomy versus transurethral prostate resection: a cost analysis. J Urol. 2010 Apr;183(4):1469–73.
- Woo H, Reich O, Bachmann A, et al. Outcome of GreenLight HPS 120W laser therapy in specific patient populations: those in retention, on anticoagulants, and with large prostates (≥ 80 ml). Eur Urol. 2008;7(Suppl):378–83.
- Data on file with Boston Scientific.
- Law KW, Tholomier C, Nguyen DD, et al. Global Greenlight Group: largest international GreenLight experience for benign prostatic hyperplasia to assess efficacy and safety. World J Urol. 2021 Apr 10. Online ahead of print.
- Malek R. Photoselective KTP Laser Vaporization of Obstructive BPH (PVP). In: Baba S, Ono Y (editors). Interventional Management of Urological Diseases. Recent Advances in Endourology, vol 8. Springer 2006. 103–22.
- Azizi M, Tholomier C, Meskawi M, et al. Safety, perioperative, and early functional outcomes of vapor incision technique using the GreenLight XPS 180W system: Direct comparison with photoselective vaporization of the prostate. J Endourol. 2017 Jan;31(1):43–9.
- National Institute of Diabetes and Digestive and Kidney Diseases. Prostate Enlargement (Benign Prostatic Hyperplasia). Accessed July 19, 2021.
- Parsons JK, Dahm P, Köhler TS, et al. Surgical management of lower urinary tract symptoms attributed to benign prostatic hyperplasia: AUA Guideline Amendment 2020. J Urol. 2020 Oct;204(4):799–804.
- Gravas S, Cornu JN, Drake MJ, et al. EAU guidelines on management of non-neurogenic male lower urinary tract symptoms (LUTS), incl. benign prostatic obstruction (BPO). 2018. https://uroweb.org/wp-content/uploads/EAU-Guidelines-on-the-Management-of-Non-neurogenic-Male-LUTS-2018-large-text.pdf.
- Ajib K, Mansour M, Zanaty M, et al. Photoselective vaporization of the prostate with the 180-W XPS-Greenlight laser: Five-year experience of safety, efficiency, and functional outcomes. Can Urol Assoc J. 2018 Jul;12(7):E318–E324.
- Montorsi F, Naspro R, Salonia A, et al. Holmium laser enucleation versus transurethral resection of the prostate: results from a 2-center, prospective, randomized trial in patients with obstructive benign prostatic hyperplasia. J Urol. 2004;172(5 Pt 1):1926–9.
- Cho MC, Park JH, Jeong MS, et al. Predictor of de novo urinary incontinence following holmium laser enucleation of the prostate. Neurourol Urodyn. 2011 Apr;30(7):1343–9.
- Misraï V, Faron M, Guillotreau J, et al. Assessment of the learning curves for photoselective vaporization of the prostate using GreenLight™ 180-Watt-XPS laser therapy: defining the intra-operative parameters within a prospective cohort. World J Urol. 2014 Apr;32(2):539–44.
Caution: U.S. Federal law restricts this device to sale by or on the order of a physician.
IMPORTANT INFORMATION: These materials are intended to describe common clinical considerations and procedural steps for the use of referenced technologies but may not be appropriate for every patient or case. Decisions surrounding patient care depend on the physician’s professional judgment in consideration of all available information for the individual case.
Boston Scientific (BSC) does not promote or encourage the use of its devices outside their approved labeling. Case studies are not necessarily representative of clinical outcomes in all cases as individual results may vary.
Results from case studies are not necessarily predictive of results in other cases. Results in other cases may vary.
Kevin Zorn, M.D., is a Boston Scientific consultant and was compensated for his contribution to this article.
All trademarks are the property of their respective owners.
Images provided courtesy of Canadian Journal of Urology.