Boston Scientific accounts are for healthcare professionals only.

David Robbins, M.D.a

Ricardo R. Gonzalez, M.D.b

Rahul Mehan, M.D.c
Editorial commentary
The sentiments expressed within this article are representative of the opinions and experiences of the respective physicians. Drs. Robbins, Gonzalez and Mehan are Boston Scientific consultants and were compensated. Physician experience and patient responses can and do vary.
Urologists Dr. David Robbins, Dr. Ricardo Gonzalez and Dr. Rahul Mehan provided their perspectives and experiences when using the GreenLight XPS™ Laser Therapy System for patients requiring further intervention following a UroLift™ procedure.
The UroLift System is commonly used to treat benign prostatic hyperplasia (BPH) and involves the use of implants to hold open the obstructed pathway blocking urine flow. UroLift offers rapid and significant improvements in symptoms, urinary flow and quality of life sustained through five years, and patients can preserve sexual function.1 UroLift is indicated for the treatment of symptoms due to urinary outflow obstruction secondary to BPH, including lateral and median lobe hyperplasia, in men 45 years of age or older. It is contraindicated for patients with a prostate volume of >100 cc. The American Urological Association (AUA) Guidelines recommend UroLift for patients with Lower Urinary Tract Symptoms (LUTS)/BPH with prostate volume 30–80 cc and verified absence of an obstructive middle lobe.2 In some cases, patients experience a reoccurrence of symptoms and require further treatment to manage their BPH. In the pivotal trial, UroLift patients had a 13.6% surgical retreatment rate and 10.7% medical retreatment rate at five years.1
Therapy with GreenLight is proven to effectively and safely treat a broad spectrum of BPH patients, including those at high risk (e.g., larger prostate, older age, greater comorbidities) and on anti-coagulants, while providing long-term durability, reduced bleeding, and shorter hospitalization and catheter times as compared to transurethral resection of the prostate (TURP).3–5 GreenLight provides durable results and symptom relief for patients.6
According to the Instructions for Use for both devices, following are important considerations for both treatments:
Q&A with Dr. Mehan and Dr. Robbins
Dr. Mehan: There are many reasons why patients would choose UroLift to treat their BPH, including that it can be performed in office under local anesthesia and the return to normal voiding is rapid.2 Additionally, sexual function is preserved, and symptom improvement is rapid and significant. Finally, there is minimal risk with the procedure, and it doesn’t negate the option for future treatment options if they are needed.2
Typically, optimal patient candidates for UroLift have a prostate volume of less than 80 cc when not on medical therapy, with International Prostate Symptom Score (IPSS) ≥ 12 with associated bother, and a Qmax (peak flow rate) less than 15 mL/s.1
Dr. Robbins: When I’m choosing patients for BPH surgery, I find out what their goals and needs and wants are as far as ejaculatory maintenance. Additionally, I assess their physical condition to determine key factors such as how much obstruction they have, how big their prostate is, what does the bladder look like, do they have a median lobe, etc. For a UroLift candidate, I’m looking for smaller prostates, and patients who are not in retention and are interested in ejaculatory preservation.2
[In the pivotal trial, UroLift patients had a 13.6% surgical retreatment rate and 10.7% medical retreatment rate at five years.1]
Dr. Gonzalez: I specialize in voiding dysfunction, and I see men who need treatments for their BPH daily — between 8 and 10 per week. Of these patients, one or two are candidates for minimally invasive surgical therapy (MIST) procedures in my particular practice.
I usually treat at least one patient a week who has had prior UroLift intervention and, for those, I tend to do laser procedures. It allows me more versatility because I can treat different shapes and morphologies of prostates, and I tend to lean on those therapies for most men.
I do not feel that UroLift is necessarily a bad option, but it may have been too little too late for these particular patients, and not enough to solve their problem.
Dr. Gonzalez: My patients who present with prior UroLift and now are considering reintervention generally are doing so because either their original symptoms persist or they appear to have been exacerbated. Some examples include patients who have smaller prostates that might have primary bladder neck obstruction or a puckered appearance of the bladder neck.
Other patients present because the degree of improvement that they experience was not to their expectation or was not good enough to allow them to be able to stop medical therapy.
Dr. Robbins: I don’t see a lot of patients who have had UroLift and who have major complications from the implants. Some patients just don’t have the relief that they expected they would have. They’re continuing to have the typical BPH symptoms of urinary urgency, frequency, they’re waking up at night, they’re straining to urinate.
Dr. Mehan: I absolutely love utilizing GreenLight for UroLift reinterventions. It is the most versatile treatment option I offer in my practice. It allows me to open the central tissue and better address the lateral lobes. I can also take down high riding bladder necks or median bars very easily and efficiently. From a patient standpoint, it avoids the risks of erectile dysfunction as seen with the TURP procedure.4 Also, with the ejaculatory hood sparing technique, ejaculatory function can better be preserved.9
Dr. Gonzalez: What I love about GreenLight is the versatility of the laser. With that single laser technology, I can do a simple incision of the prostate. I can vaporize the prostate or perform an enucleation of the prostate with a safe technology that minimizes bleeding.3 When I have a patient who has a tight bladder neck or high median bar, and who hopes to preserve as much ejaculatory function as possible, making an incision of the prostate with GreenLight is effective and can have an antegrade ejaculation rate of 85%.10
In patients who have bulky obstruction by the lateral lobes, photo-selective vaporization (PVP) and enucleation techniques along with vaporization incision technique (VIT) with GreenLight allows resection of the obstructing tissue as well as the UroLift clips, and allows us to remove the obstruction, thereby improving the patient’s ability to void the bladder, and impact their quality of life.4 Also, in patients who had an obstructing median lobe, you can enucleate the median lobe and enucleate the lateral lobes. Or you can enucleate the median lobe and vaporize the lateral lobes. The benefit is that the same laser allows you to employ different techniques where needed within the prostate.
And these techniques are not solely exclusive. For example, one man may only have vaporization or one man may only have enucleation. In the same patient you can enucleate one lobe, but vaporize two lobes, or enucleate two lobes and vaporize one lobe. Because GreenLight is versatile enough that it lets you employ the technique you need to solve the problem, and I think of it as my Swiss Army knife in my arsenal for BPH.
And not only allowing me to treat different shapes and sizes, but also higher risk men who are perhaps anticoagulated or who are just delicate enough that I would not want to do a type of procedure like a TURP where the patient might need to stay the night in the hospital.5 As much as possible, I really want to do day surgery and have a patient go home the same day to keep them out of the hospital. In the U.S., GreenLight can be a same-day procedure.11 This helps to avoid exposing them to risks that may be inherent from a hospital stay, but also keeps us from using hospital resources that we don’t have to use.
Dr. Robbins: GreenLight is a great solution because here in the U.S., it can be a day surgery procedure with minimal catheterization time, bleeding and recovery.11,12 Additionally, with GreenLight you can remove the UroLift implants.
As a treatment in and of itself, GreenLight is really definitive — you can actually take away or vaporize the majority of the obstructing tissue. You can remove the median lobe and the UroLift implants and create a nice open channel for the patient to void through and have significant relief of their symptoms.
Dr. Mehan: I have found GreenLight to be an invaluable part of my BPH treatment tool bag. It is the jack of all trades and works well with both small and large prostates. GreenLight has proven durability. It is clinically proven to be comparable in IPSS, Qmax, symptoms relief and long-term durability to TURP with a better safety profile.3 In my practice, I have found that patients want to minimize their risk of sexual side effects and often choose MIST procedures for that. If a MIST procedure is not right, or if they have failed a MIST procedure, GreenLight is the next logical choice. It has replaced TURP in my practice. Over my last 1,000 cases, I have sent nearly all patients home after the procedure.
Dr. Gonzalez: If I have a man with BPH and urinary symptoms who is responsive to medicine, and they feel it is helping their urinary symptoms, but they do not want to be dependent on a medicine, then I think they’re excellent candidates for a MIST procedure like Rezūm™ Water Vapor Therapy, UroLift or iTIND. The next step would be to measure the size of their prostate. If their prostate is 30 to 80 grams, they remain a candidate for a MIST procedure.2 If, on anatomical study with ultrasound and cysto, we see that they have an intravesical median lobe, then it is my preference to offer that patient Rezūm Therapy. But if they don’t have a median lobe and it’s just lateral lobe obstruction from 30 to 80 grams, that patient who’s responding to medical therapy, then it’s up to the patient to choose between UroLift, Rezūm Therapy and iTIND.2
If I have a patient who has urinary symptoms that are not alleviated by medical therapy, I do not offer them a MIST procedure because the degree of improvement with a MIST procedure would not be enough. The IPSS improvement I expect to have from a MIST procedure, is minimum of 8 points and up to an 11-point improvement. But with surgery, in my experience, we can get a 15+ point improvement. So 16, 17 points is not unheard of after GreenLight enucleation or vaporization.
In patients who have severe symptoms, if a patient has an IPSS score of 30, despite having a prostate in the 30 to 80 range, it is very unlikely that a MIST procedure alone would get that patient to have mild symptoms because in my practice, the average patient has improvement of 8 to 11 points. We can really normalize them with doing something like a laser vaporization or laser enucleation with GreenLight.
If a patient has a prostate over 80 grams, then in my practice we move into treatment options for larger prostates vs. reaching for MIST procedures. In those cases, I offer these patients options like laser enucleation or ablation of the prostate, which are newer therapies with fewer side effects than TURP.
The absolute indications for surgeries, as opposed to MIST procedures, remain the same on the AUA and EAU guidelines, which are urinary retention, bladder stones, recurring hematuria, recurring infections, renal failure, and failure of medical therapy.1,13
What I like about GreenLight is that it’s a one-size-fits-all treatment modality that I can use for a large prostate, small prostate, median lobe, no median lobe, lateral obstruction. The other modalities come in when patients have certain needs and desires, such as office-based procedures and a strong interest in ejaculatory preservation, and they have a smaller prostate that is most likely to result in a positive clinical outcome with a MIST procedure.
Dr. Mehan: My advice to interested other urologists, is to give it a try. If you have taken one new BPH treatment modality, why not try another? There is a renaissance of new technology and it’s beautiful. Patients want innovation. GreenLight is easy to onboard and gives you an option to treat men when MIST treatments are not ideal or fail. GreenLight can enhance outcomes and in my opinion, provides an improved patient and provider experience.14
Dr. Gonzalez: I would like my colleagues to know that, with GreenLight laser therapy, whether it’s vaporization, the vaporization incision technique, or enucleation, which we have been doing for almost two decades, we know it is safe, reliable, and that the re-treatment rate is 4.8% at five years, making it very durable.15 I like laser therapy because it allows me to safely treat patients with multiple shapes and sizes of prostate and with multiple comorbidities, such as patients with health conditions requiring anticoagulation, or higher risk populations, often as an outpatient.4,5
In terms of durability you have to consider debulking tissue to be the most durable sort of the gold standard, and I prefer the GreenLight laser over TURP, because you’re going to achieve what TURP can achieve, if not more, but with shorter catheterization times, most likely no hospital stay and less bleeding.3 That’s what makes GreenLight wonderful.
Dr. Gonzalez: I would encourage them to have something in their arsenal that allows them to treat a broad spectrum of patients who are walking in the door with urinary problems. As men age, we know they’re more likely to have multiple health conditions and more likely to have urinary tract symptoms associated with prostate enlargement. Most patients we’re going to see who have BPH with obstruction are going to be older and many will be high risk (e.g., larger prostate, older age, greater comorbidities). So having something in your arsenal that allows you to treat those men, as well as being able to salvage maybe a healthier man or other men who didn’t respond to something less invasive is very versatile and useful. So again, I consider it the Swiss Army knife of my BPH arsenal.
Dr. Robbins: For my colleagues who really want to treat BPH, GreenLight really has to be part of their tool belt. The most recent version of GreenLight XPS has been around for a long time and is proven to be able to debulk tissue in a safe and minimally invasive manner.3
Conclusion
The participating urologists agree that GreenLight can be a tool of choice for treating patients who may need reintervention following UroLift due to the versatility and durability of the therapy while also providing enhanced outcomes for patients.3
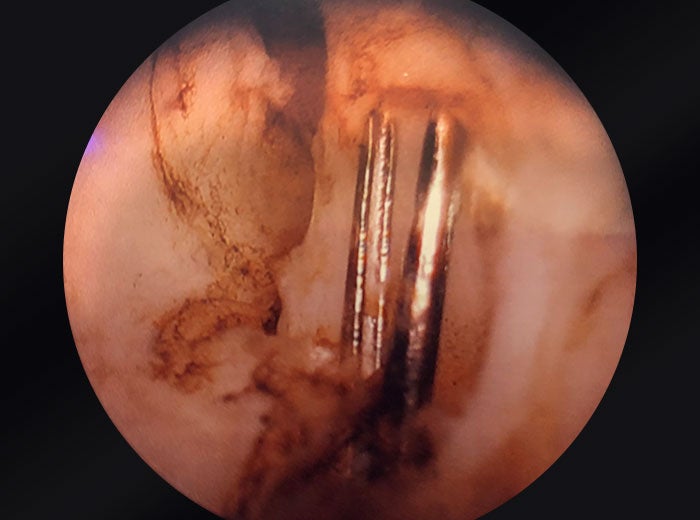
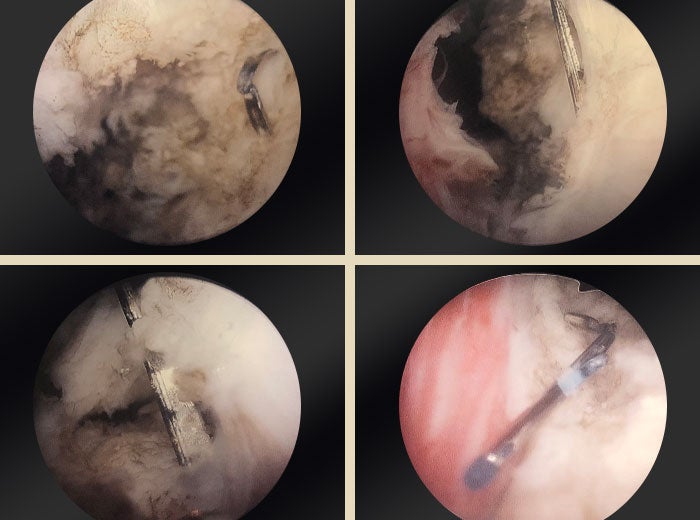
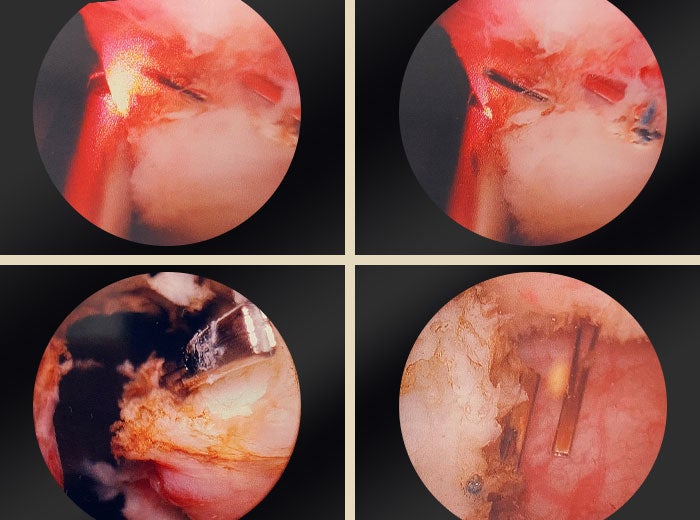
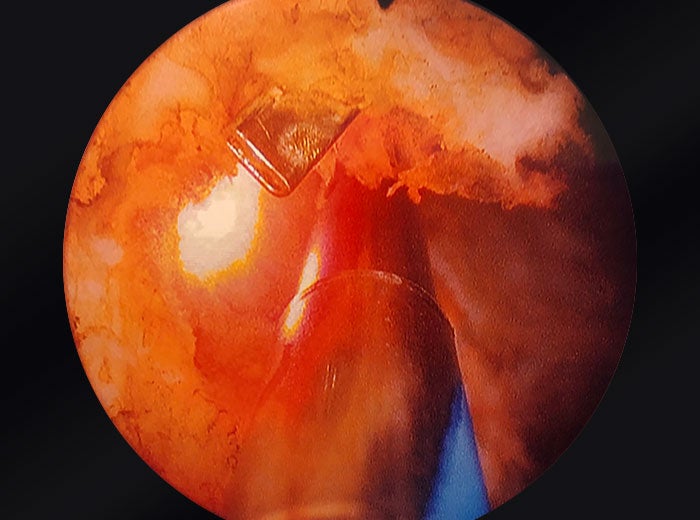
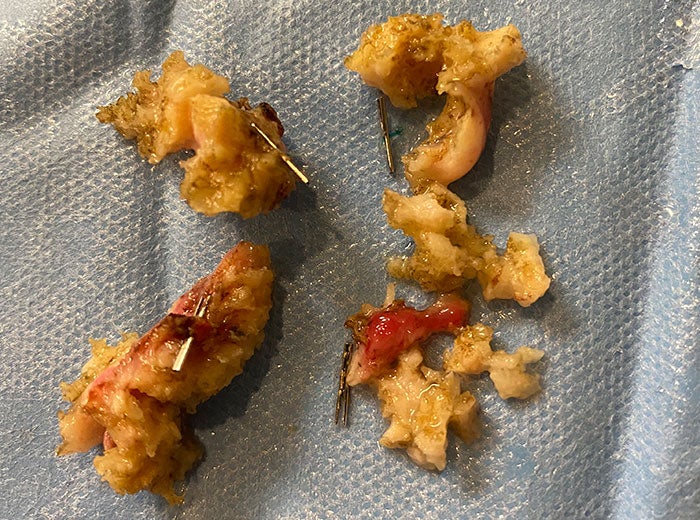
A step-by-step overview of using GreenLight to treat UroLift patients
Dr. Ricardo R. Gonzalez
UroLift clips embedded in prostatic tissue
Images provided courtesy of Dr. Ricardo Gonzalez.
Related content
*Results from different clinical investigations are not directly comparable. Information provided for educational purposes only.
aUrological Consultants of Florida, P.A.
bAssociate Professor of Urology, Houston Methodist Hospital. Adjunct Associate Professor of Urology, Texas A&M College of Medicine
cFounder, East Valley Urology Center
References
- Roehrborn CG, Barkin J, Gange SN, et al. (2017). Five year results of the prospective randomized controlled prostatic urethral L.I.F.T. study. Can J Urol. 2017 Jun;24(3):8802–13.
- Lerner LB, McVary, KT, Barry MJ, et al.: Management of lower urinary tract symptoms attributed to benign prostatic hyperplasia: AUA Guideline part I, initial work-up and medical management. J Urol. 2021 Oct;206(4):806–17.
- Thomas JA, Tubaro A, Barber N, et al. A multicenter randomized noninferiority trial comparing GreenLight-XPS laser vaporization of the prostate and transurethral resection of the prostate for the treatment of benign prostatic obstruction: Two-yr outcomes of the GOLIATH study. Eur Urol. 2016 Jan;69(1):94–102.
- Lai S, Peng P, Diao T, et al. Comparison of photoselective green light laser vaporisation versus traditional transurethral resection for benign prostate hyperplasia: an updated systematic review and meta-analysis of randomised controlled trials and prospective studies. BMJ Open. 2019 Aug 21;9(8):e028855.
- Rajih E, Tholomier C, Hueber PA, et al. Evaluation of surgical outcomes with photoselective GreenLight XPS laser vaporization of the prostate in high medical risk men with benign prostatic enlargement: a multicenter study. J Endourol. 2017 Jul;31(7):686–93.
- Bachmann A, Tubaro A, Barber N, et al. 180-W XPS GreenLight laser vaporization versus transurethral resection of the prostate for the treatment of benign prostatic obstruction: 6-month safety and efficacy results of a European multicentre randomised trial—the GOLIATH study. Eur Urol. 2014 May;65(5):931–42.
- GreenLight Instructions for Use.
- UroLift Instructions for Use: https://f.hubspotusercontent30.net/hubfs/2618738/Brochures_Forms/L00181-01_RevA_UroLift%20_System_UL400_IFU_US.pdf.
- Abolazm AE, El-Hefnawy AS, Laymon M, et al. Ejaculatory hood sparing versus standard laser photoselective vaporization of the prostate: sexual and urodynamic assessment through a double blinded, randomized trial. J Urol. 2020 Apr;203(4):792–801.
- Kini M, Te AE, Kashanian JA, et al. Ejaculatory hood-sparing photoselective vaporization of the prostate vs bipolar button plasma vaporization of the prostate in the surgical management of benign prostatic hyperplasia. J Endourol. 2020 Mar;34(3):322–9.
- Goh AC, Gonzalez RR. Photoselective laser vaporization prostatectomy versus transurethral prostate resection: A cost analysis. J Urol. 2010 Apr;183(4):1469–73.
- Cornu JN, Ahyai S, Bachmann A, et al. A systematic review and meta-analysis of functional outcomes and complications following transurethral procedures for lower urinary tract symptoms resulting from benign prostatic obstruction: an update. Euro Urol. 2015 Jun;67(6):1066–96.
- Gravas S, Cornu JN, Gacci M, et al. EAU Guidelines on Management of Non-Neurogenic Male Lower Urinary Tract Symptoms (LUTS), incl. Benign Prostatic Obstruction (BPO). Update March 2022. https://uroweb.org/guidelines/management-of-non-neurogenic-male-luts.
- Capitán C, Blázquez C, Martin MD, et al. GreenLight HPS 120-W laser vaporization versus transurethral resection of the prostate for the treatment of lower urinary tract symptoms due to benign prostatic hyperplasia: A randomized clinical trial with 2-year follow-up. Eur Urol. 2011 Oct;60(4):734–9.
- Calves J, Thoulouzan M, Perrouin-Verbe MA, et al. Long-term patient-reported clinical outcomes and reoperation rate after photovaporization with the XPS-180W GreenLight laser. Eur Urol Focus. 2019 Jul;5(4):676–80.
Caution: U.S. Federal law restricts this device to sale by or on the order of a physician.
IMPORTANT INFORMATION: These materials are intended to describe common clinical considerations and procedural steps for the use of referenced technologies but may not be appropriate for every patient or case. Decisions surrounding patient care depend on the physician’s professional judgment in consideration of all available information for the individual case.
Boston Scientific (BSC) does not promote or encourage the use of its devices outside their approved labeling. Case studies are not necessarily representative of clinical outcomes in all cases as individual results may vary.
Results from case studies are not necessarily predictive of results in other cases. Results in other cases may vary.
Results from different clinical investigations are not directly comparable. Information provided for educational purposes only.
For information purposes only. The content of this article/publication is under the sole responsibility of its author/publisher and does not represent the opinion of BSC.
The sentiments expressed within this article are representative of the opinions and experiences of the respective physicians. Drs. Robbins, Gonzalez and Mehan are Boston Scientific consultants and were compensated. Physician experience and patient responses can and do vary.
All images are courtesy of Dr. Gonzalez. All trademarks are the property of their respective owners.
All trademarks are the property of their respective owners.