Boston Scientific accounts are for healthcare professionals only.

ANGIOJET™ Peripheral Thrombectomy System
Reimbursement
Configure or select a product to continue to order
- Overview
- Venous
- Arterial
- Technical specifications
- Ordering information
- Clinical outcomes
- Case studies
- Training
Features & benefits
The AngioJet Thrombectomy system provides the power and flexibility for rapid thrombus removal.
Active aspiration and Power Pulse lytic delivery for tough clots
Wide offering of catheters for treating arterial, venous and AV access in vessels ranging from 1.5 mm to large iliofemoral clot burdens
- Provides quick restoration of blood flow, symptom improvement and ease of use
AngioJet console overview
Advanced, user-friendly console
- Control system automates set-up and monitors operation
- Step-by-step interface for procedural efficiency
- Automated system self-configures to each catheter
- Compact, highly mobile console

Technical assistance
For technical assistance or to inquire about the purchase of a console please contact (800) 949-6708
How AngioJet works
Mechanism of action
- The AngioJet console monitors and controls the system.
- The console energizes the pump which sends pressurized saline to the catheter tip.
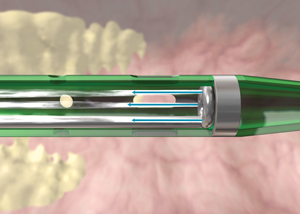
3. Saline jets travel backwards to create a low pressure zone causing a vacuum effect.
(Image 1)
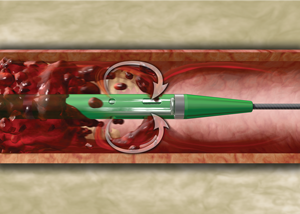
4. Thrombus is drawn into the in-flow windows and the jets push the thrombus back down the catheter.
(Image 2)

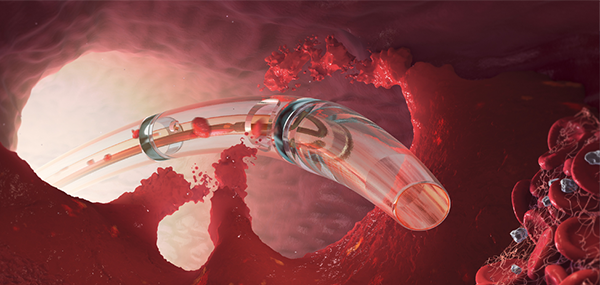
5. Thrombus is evacuated from the body and into the collection bag.
(Image 3)
DVT Thrombectomy
ZelanteDVT catheter
The AngioJet ZelanteDVT thrombectomy catheter is specifically designed to treat deep vein thrombosis (DVT) in large-diameter upper and lower peripheral veins ≥ 6 mm. ZelanteDVT is the most powerful thrombectomy catheter in the market-leading AngioJet portfolio.
The ZelanteDVT catheter makes it possible to quickly remove large thrombus burden in veins and restore blood flow, giving you the power to dominate DVTs.
- Four times the thrombus-removal power of Solent™ Omni and Solent Proxi catheters**
- Single inflow window for torqueable and directional thrombectomy power
- Power Pulse enabled for infusion of physician-specified fluids, including thrombolytic agents
- Inflow window indicator band
The 8 F ZelanteDVT catheter
The Need to More Efficiently Treat Large Vein Thrombus: Conceptualizing the AngioJet ZelanteDVT Catheter
See real-world use cases of AngioJet in a variety of venous procedures.
Solent Omni and Proxi catheters
The Solent Omni and Proxi catheters provide the power and flexibility to remove thrombus in veins ≥ 3 mm. Power Pulse Delivery can infuse lytic into the clot. Contrast injection capability and guidewire exchange increase treatment efficiencies.
Venous catheter specifications
| ZelanteDVT | Solent Omni | Solent Proxi | |
|---|---|---|---|
| System Compatibility | Ultra | Ultra | Ultra |
| Vessel Diameter | ≥ 6 mm | 3 mm | 3 mm |
| Working Length | 105 cm | 120 cm9 | 0 cm |
| Shaft Diameter | 8 F | 6 F | 6 F |
| Double Marker Band | 15 mm | N/A | N/A |
| Guidewire Compatibility | 0.035” | 0.035" | 0.035" |
| Sheath Compatibility | 8 F | 6 F | 6 F |
AV Access Thrombectomy
Thrombus narrowing or restricting flow within AV access fistulas and grafts can prevent a patient from undergoing life supportive dialysis treatment.
Used for thrombectomy of both synthetic grafts and natural fistulae, the AngioJet System utilizes powerful Cross-Stream technology to remove thrombotic materials from the dialysis access conduit with minimal vessel wall trauma, potentially decreasing the risk for future thrombotic events.
Catheters with AV access indication include: AVX™, Solent Proxi and Solent Omni
Clinical data
The AngioJet Thrombectomy System provides the power and flexibility to remove venous thrombus and restore flow in the most challenging of DVT cases.
For deep vein thrombosis cases, the PEARL Registry data demonstrated:
- 34% of patients were treated in a single session
- 75% of procedures were completed in < 24 hours
- Less total lytic dose for treating DVT when using PowerPulse/Rapid Lysis (with/without CDT) versus CDT alone
Presented by Dr. Ali Amin at Charing Cross 2014; Final PEARL Data
AngioJet ZelanteDVT was not studied in the PEARL Registry. Presented by Dr. Mark Garcia at CIRSE 2013; Final PEARL Data Aug 2013
**When compared to current AngioJet catheters. Bench test data on file. Bench test results may not necessarily be indicative of clinical performance.
All trademarks are the property of their respective owners.
Arterial Thrombectomy
AngioJet Thrombectomy removes thrombus burden from arterial vessels as small as 1.5mm - quickly restoring flow and resolving symptoms to enable the culprit lesion to be exposed and treated.
Arterial catheter specifications
| Solent Omni | Solent Proxi | Solent Dista | |
|---|---|---|---|
| System Compatibility | Ultra | Ultra | Ultra |
| Vessel Diameter | 3 mm | 3 mm | 1.5 mm |
| Working Length | 120 cm | 90 cm | 145 cm |
| Shaft Diameter | 6 F | 6 F | 4 F / 3 F |
| Guidewire Compatibility | 0.035" | 0.035" | 0.014" |
| Sheath Compatibility | 6 F | 6 F | 4 F |
Want to learn more? See Arterial case studies
Clinical data
For Limb Ischemia cases, the PEARL registry data demonstrated:
- 89% limb salvage rate
- 56% of patients were treated in a single session
- 80% of procedures were completed in <24 hours
Presented by Dr. Ali Amin at Charing Cross 2014; Final PEARL Data
Technical information
Catheter specifications
| Model | Indication | Delivery Platform | Minimum Vessel Diameter | Catheter Length | Catheter Diameter | Guidewire | Power Pulse™ Enabled | Guidewire Swappable | Contrast Injection Port |
|---|---|---|---|---|---|---|---|---|---|
| ZelanteDVT™ | Venous | OTW | 6 mm | 105 cm | 8 F | 0.035” | Yes | Yes | Yes |
| Solent™ Omni | Peripheral Arterial and Venous, AV Access | OTW | 3 mm | 120 cm | 6 F | 0.035” | Yes | Yes | Yes |
| Solent™ Proxi | Peripheral Arterial and Venous, AV Access | OTW | 3 mm | 90 cm | 6 F | 0.035” | Yes | Yes | Yes |
| Solent™ Dista | Peripheral Arterial | OTW | 1.5 mm | 145 cm | 4 F / 3 F | 0.014” | Yes | N/A | N/A |
| AVX™ | AV Access Grafts and Fistula | OTW | 3 mm | 50 cm | 6 F | 0.035” | N/A | N/A | Yes |
Ordering information
| Product Name | Catalog Number | UPN |
|---|---|---|
| AngioJet System Console | 105650 | 105650-001 |
| ZelanteDVT™ | 114610 | 114610-001 |
| Solent™ Omni | 109681 | 109681-001 |
| Solent™ Proxi | 109676 | 109676-001 |
| Solent™ Dista | 111303 | 111303-001 |
| AVX™ | 105039 | 105039-001 |
| Power Pulse Delivery Kit (5 per box) | 104834 | 104834-0021 |
AngioJet clinical outcomes
PEARL registry overview
Study design
PEARL I followed patients for 3 months with documentation of symptomatic improvement after AngioJet thrombectomy (with mid-length catheters).
PEARL II followed patient outcomes through 12 months after AngioJet thrombectomy with any AngioJet catheter.
- All patients were treated with AngioJet Thrombectomy
- Patient history, procedural information, adjunctive treatments, outcomes and adverse events were collected
- Patients were analyzed in arterial, venous & dialysis access indications
Objectives
- Determine efficacy of thrombus removal from baseline to final angiogram/venogram
- Evaluate clinical outcomes of treated patients at defined intervals of 3, 6 & 12 months
- Characterize clinical events
- Characterize treatment options used with the AngioJet System
- Estimate rate of AngioJet Thrombectomy-related adverse events
PEARL I Followed patients for 3 months with documentation of symptomatic improvement after AngioJet thrombectomy (with mid-length catheters).
PEARL II Followed patient outcomes through 12 months after AngioJet thrombectomy with any AngioJet catheter.
- All patients were treated with AngioJet Thrombectomy
- Patient history, procedural information, adjunctive treatments, outcomes and adverse events were collected
- Patients were analyzed in arterial, venous & dialysis access indications
Enrollment
952 patients, 34 enrolling sites, 4 countries
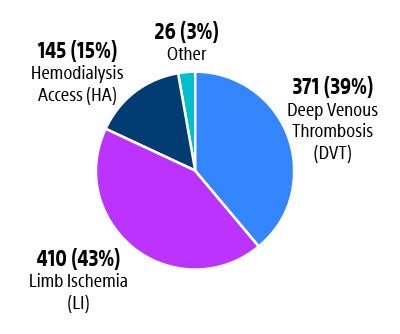
N=371 patients
PEARL DVT
Summary
- 34% of patients treated in single session; 87% of patients had 2 or less lab sessions
- 38% of procedures treated in ≤ 6 hours; 75% completed in ≤ 24 hours
- Less total lytic use when delivered utilizing AngioJet (Power Pulse and/or Rapid Lysis) than if CDT were included in treatment with final venographic results comparable across all technique subgroups
- 1295 venous vessels treated with 97% showing improvement, 3% unchanged, <1% worse
Venographic results
by Technique Subgroups (p<0.0001) N=1295 vessels treated
- Amongst the 4 treatment groups there wasn’t any statistical difference in baseline occlusion, final occlusion or in the change of occlusion.
- The difference seems to be in the treating physician’s preference to treatment.
Venographic results
by technique subgroups (p<0.0001) N=1295 vessels treated
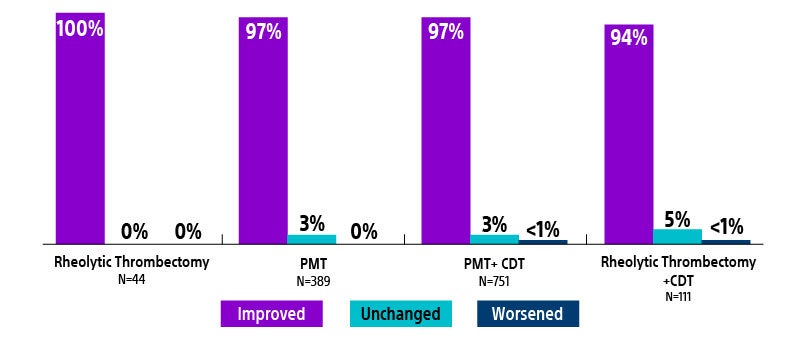
CDT = catheter-directed thrombolysis
PMT = pharmacochemical thrombolysis
Presented by Dr. Mark Garcia at CIRSE 2013; Final PEARL Data
N=410 patients
PEARL limb ischemia
Summary
- 947 arterial vessels treated with 93% showing improvement, 6% unchanged, <1% worse
- 89% limb salvage rate (185/207). 207 ALI patients had a baseline Rutherford Classification of lla, llb and lll
- 56% of patients treated in single session; 86% of patients had 2 or less lab sessions
- 58% of procedures treated in < 6 hours; 80% completed in < 24 hours
Angiographic results
by location (p<0.0001)
- Higher % of substantial lysis were achieved in the groups with PMT.
- There was a difference (p=0.0003) In the mean baseline thrombus between the 4 groups. With the PMT + CDT group having a greater occlusion initial score than the other groups.
Angiographic results
% of treated vessels by location (p<0.0001)
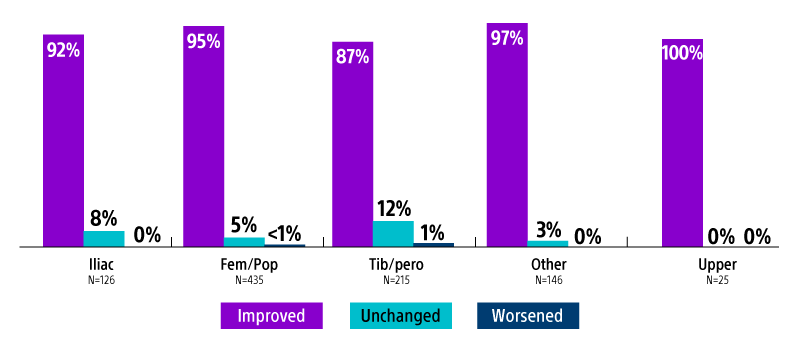
CDT = catheter-directed thrombolysis
PMT = pharmacomechanical thrombolysis
Presented by Dr. Ali Amin at Charing Cross 2014; Final PEARL Data
N=145 patients
PEARL AV access
Summary
- Hemodialysis Access Overall Patency: 78% patency at 3 months; KDOQI minimum goal is 40% at 3 months
- 76% graft/fistula survival at 1 year
Treatments utilized & subgroups
- Total 145 patients (65% grafts / 35% fistulas); 186 treated vessels
- 86% (125/145) of patients treated with AngioJet Thrombectomy without thrombolytics
Hemodialysis Access
- KDOQI: minimum goal for percutaneous thrombectomy is 40% unassisted patency and functionality at 3 months
Hemodialysis access
Overall Patency
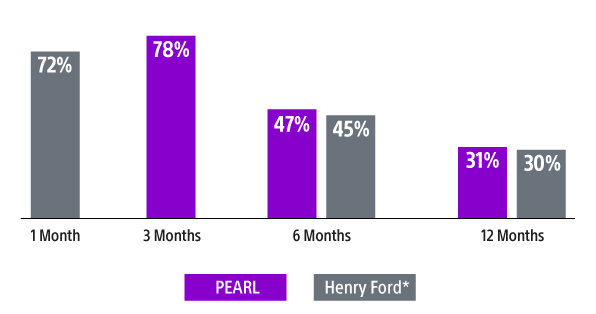
*Kakkos SK, Haddad GK, Haddad J, Scully MM. J Endovasc Ther. 2008;15(1):91-102
Simoni. PEARL Registry Hemodialysis Access. VEITH 2013
National Kidney Foundation Clinical Practice Guidelines and Recommendations; 2006
KDOQI, Kidney Disease Outcomes Quality Initiative
Presented by Dr. Eugene Simoni at VEITH 2013; Final PEARL Data
Case studies
Explore our library of Venous and Arterial cases
- Venous case studies
- Arterial case studies
Featured case
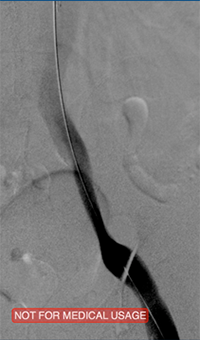
Venous thrombosis extending from popliteal to external iliac vein
Extensive DVT of the right common femoral and external iliac was treated with the 8 F AngioJet™ ZelanteDVT™ catheter.
Patient history
73 year old with 1-week old right leg swelling and pain. Started on anticoagulation and discharged.
Consult confirmed extensive DVT from popliteal extending into external iliac vein.
Procedural steps
- Power Pulse ( tPA 10 mg in 50 cc)
- Patient put on 2-hour lytic catheter drip in holding area
- Thrombectomy performed with 8F ZelanteDVT catheter
- Directional ability of ZelanteDVT allowed targeting of residual thrombus in Popliteal and Superficial Femoral Vein Post Venography shows complete resolution of thrombus
Occlusive thrombus extending into the iliac vein

Femoral vein pre-treatment
Iliac vein post-ZelanteDVT

Iliac vein post-PTA & stent
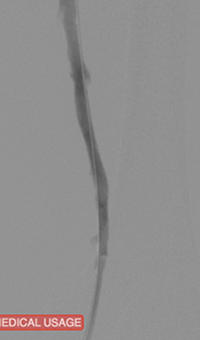
Femoral vein post-ZelanteDVT
Images courtesy of Jeffrey Y. Wang, MD FACS, Vascular Surgeon; Horizon Vascular Specialist, Maryland. November, 2015
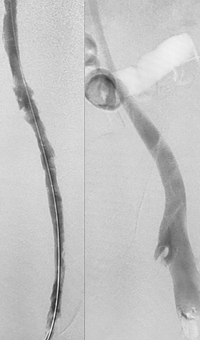
Pharmacomechanical revascularization of extensive iliofemoral thrombus
60 year old female presented with 4 weeks calf pain 1 week swelling.
Procedural steps
- Power Pulse delivery 10mg tPA
- 20 minute dwell time
- ZelanteDVT runtime 415 seconds
- Total case time 90 minutes
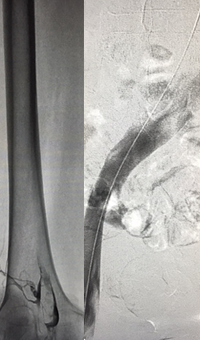
Iliofemoral thrombus pre-treatment (left) and Power Pulse delivery (right)

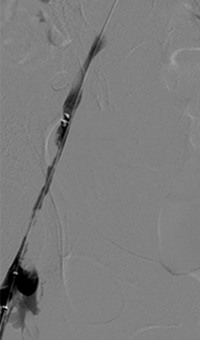
Post-ZelanteDVT Mechanical Thrombectomy
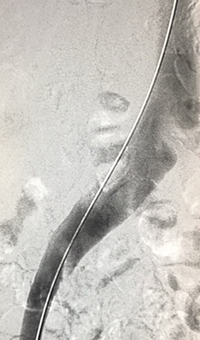
Post-ZelanteDVT runtime 415 seconds
Images Courtesy of Charles Wyble M.D. – Vascular Surgical Associates, Marietta, Georgia – January 5, 2016
Acute DVT left lower extremity revascularization
47 year old male presented with leg swelling ~2 weeks.
Procedural steps
- Power Pulse delivery of 10mg tPA followed by
- 20 minute dwell time
- Total runtime was 300 seconds

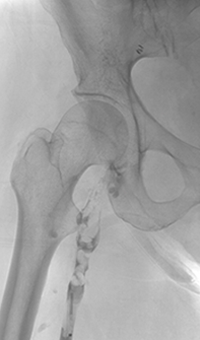
Acute Iliofemoral thrombus pre-treatment
IVC Filter placed (left image)
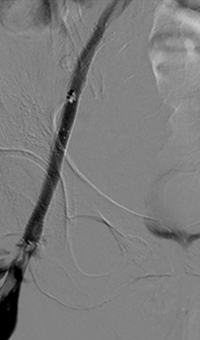
Post ZelanteDVT pharmacomechanical thrombectomy
Case images courtesy of David Wilson M.D. – Harbin Clinic, Rome, Georgia – December 19, 2015
Acute DVT left lower extremity swelling
48 year old woman with a history of metastatic cervical cancer with new left lower swelling. The patient has known intracranial aneurysm in addition to an enhancing pelvic mass.
Procedural steps
- Treatment with AngioJet Solent Omni Thrombectomy catheter
- No Power Pulse Delivery used
Pre-treatment
Thrombectomy treatment with AngioJet™ Solent™ Omni catheter
Post-treatment venogram
Treatment of May-Thurner
Pre-procedure venogram
IVC/Iliac and prox common femoral

1 pass AngioJet Solent Proxi
(Patient has not had any lytics) Distal Iliac and common femoral

Collection bag after first pass
Clot from single pass of distal iliac and common femoral
Power Pulse was used for second pass with AngioJet
Post-Power Pulse and Thrombectomy
30 minute dwell time of lytics and 3 min 10 seconds of thrombectomy
AV Access: Thrombectomy of left brachial artery-axillary vein graft
Baseline
Thrombosed AV graft with stenosis at venous anastomosis
AngioJet™ System activated
AngioJet DVX™ catheter in AV graft

Post-AngioJet thrombectomy
Imaging post-AngioJet system activation in venous side of AV graft
Final result
Imaging post-AngioJet system activation in arterial side of AV graft
AV Access: Thrombectomy of left brachiocephalic AV fistula
Baseline
Thrombosed AV Fistula. AVF had previously undergone angioplasty to treat a stenosis in the mid-part
Post-thrombectomy passes, PTA
Fistulogram following two passes with an AngioJet DVX Catheter (no thrombolytics used) and angioplasty of focal stenosis
Final result
Recoil stenosis. A stent-graft was deployed across the stenosis to maintain patency with a good result. The patient dialysed via the fistula the same day
Results from case studies are not necessarily predictive of results in other cases. Results in other cases may vary.
Case CLI with right foot ulcer thrombectomy: Posterior and anterior tibial

Arteriogram of posterior and anterior tibial post-CDT
PT and AT remained occluded following overnight CDT infusion of lytic

Post-AngioJet™ Solent™ Dista thrombectomy with PowerPulse™ delivery
AngioJet Solent Dista Catheter used in Power Pulse mode in both AT and PT. 30 min dwell in AT and 45 min dwell in PT. Followed by Solent Dista Catheter used in thrombectomy mode

Post-procedure arteriogram
Image following ballooning of small focal lesion in PT
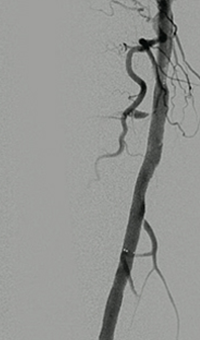
Thrombectomy of occluded SFA

Imaging SFA showing thrombus and calcification
Male in his late 40s presenting with pain in his right leg. An angiogram showed a total occlusion in the right superior femoral artery (SFA)

Solent™ Proxi catheter positioned before the lesion
The physician delivered (antegrade) the Solent Proxi catheter to the proximal margin of the occlusion

Thrombus removed following AngioJet™ treatment
After the third pass with Solent Proxi
Post-adjunctive treatment
Final angiogram showing flow post-treatment
Results from case studies are not necessarily predictive of results in other cases. Results in other cases may vary.
Training for the AngioJet System
Online medical training and education courses
The EDUCARE online platform makes healthcare education and training more relevant, more comprehensive, more personal, and more accessible. Register to access a library of procedural videos, case studies, training resources, and events.