
")

")

")
")


")
")



Patient Selection
Which Patients Should Be Considered for an S-ICD?
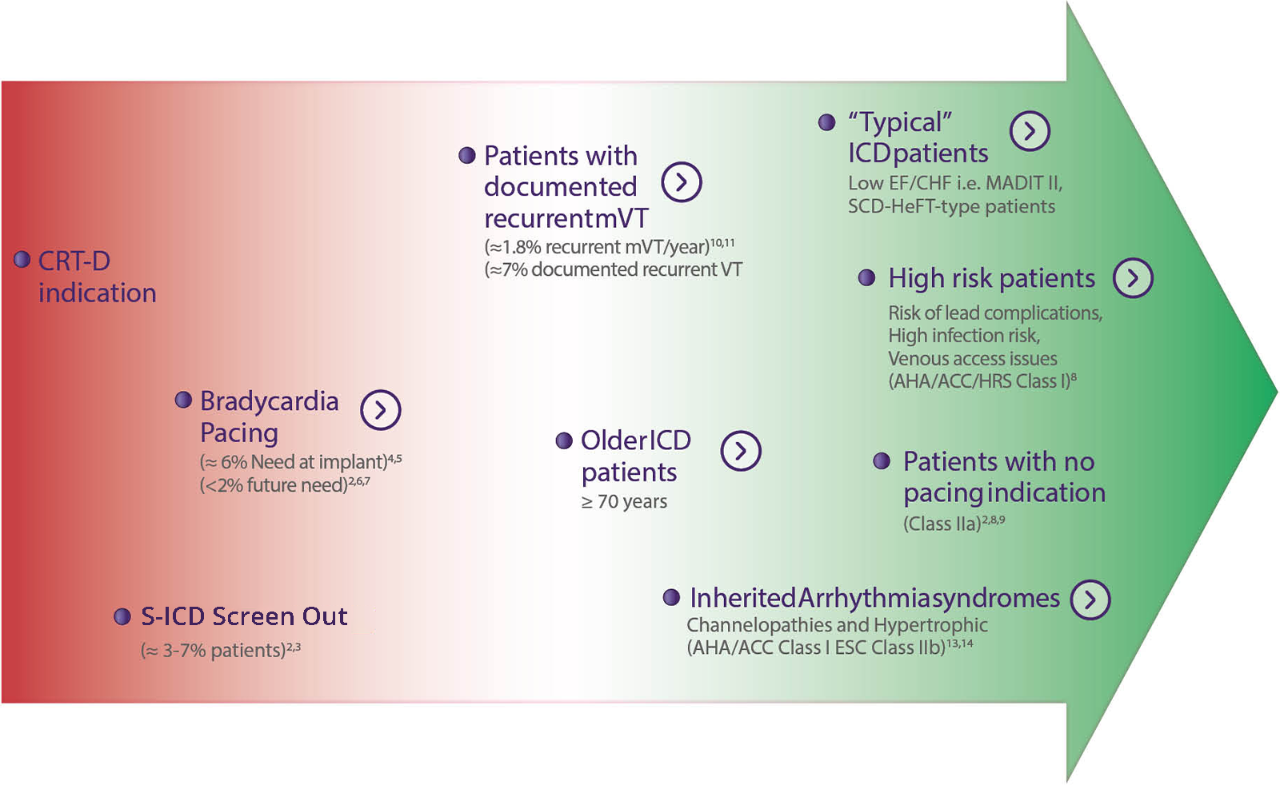
The S-ICD has been implanted with great outcomes in over 99,000 patients.1 These patients are protected from both the risk of sudden cardiac death and the risks of complications with transvenous leads. The S-ICD system is guideline recommended for the majority of ICD indicated patients without a pacing indication.


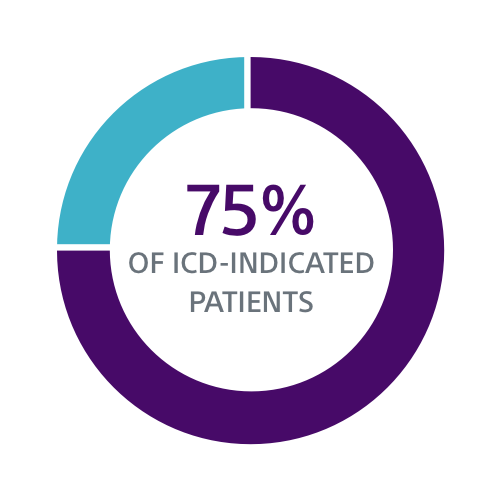
S-ICD is Guideline Recommended
Have ≥1 Comorbidity Associated
with Device Infection15-17
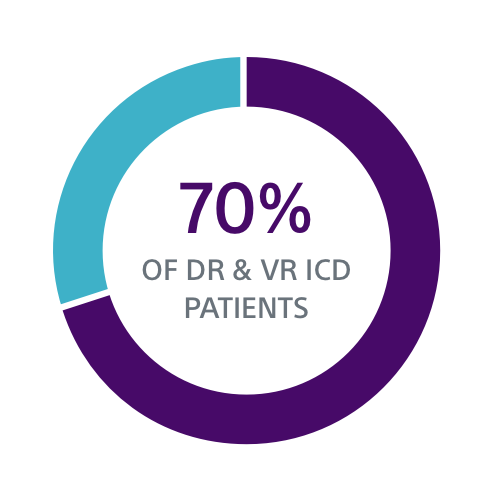
Under 75 Have No Pacing
Indication at Implant18-19
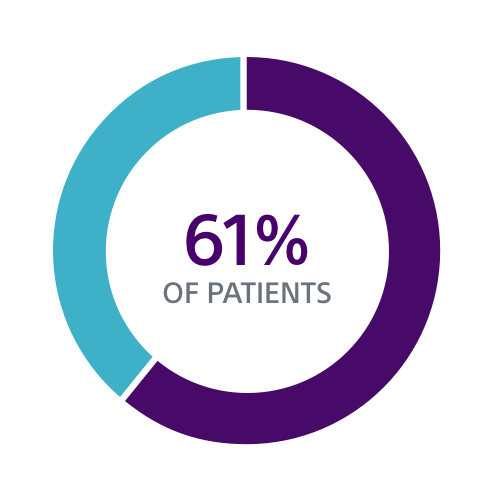
Venous Stenosis Following
Initial Device Implantation20
Clinical Data Supports S-ICD for a Broad Group of Patients
Both the PRAETORIAN and UNTOUCHED studies confirm S-ICD should be considered the first choice for all ICD-indicated patients without a pacing indication.
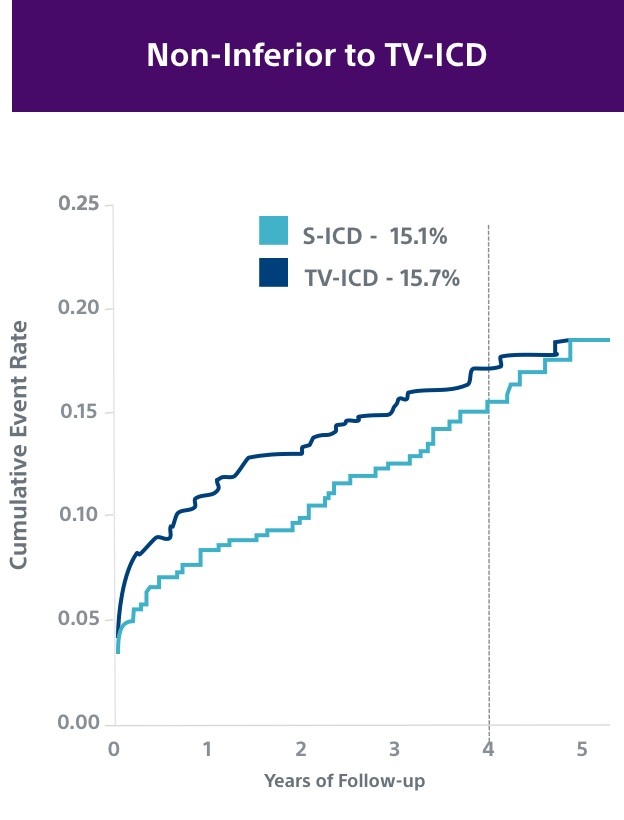
PRAETORIAN2
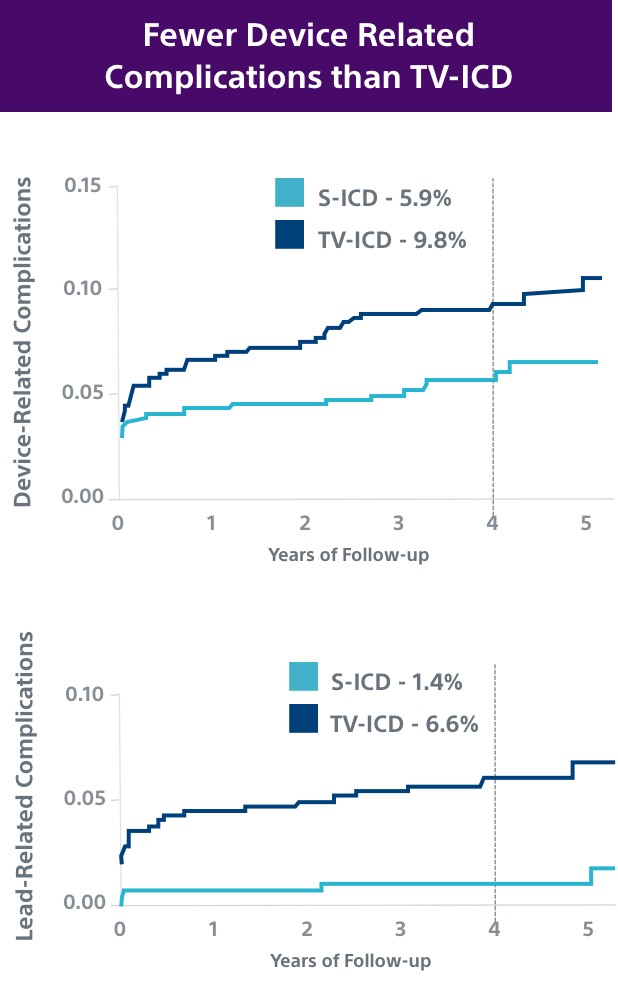
This investigator-sponsored trial demonstrated S-ICD had comparable performance to TV-ICD, despite including primarily older S-ICD devices and implant techniques. According to the PRAETORIAN study, S-ICD:
- Had significantly fewer lead-related complications (1.4% vs. 6.6%, P=0.001)
- Demonstrated fewer serious infections requiring extraction (8 TV-ICD vs. 4 S-ICD)
- Showed a trend in fewer overall complications (5.9% vs. 9.8%, P=0.11); likely to be significantly lower at 8 years in PRAETORIAN XL
UNTOUCHED6
The UNTOUCHED study demonstrated patients with EMBLEM™ MRI S-ICD with SMART Pass had a 2.4% rate of inappropriate shocks at 1 year, which is as low or lower than TV-ICD devices.2,18,21,22
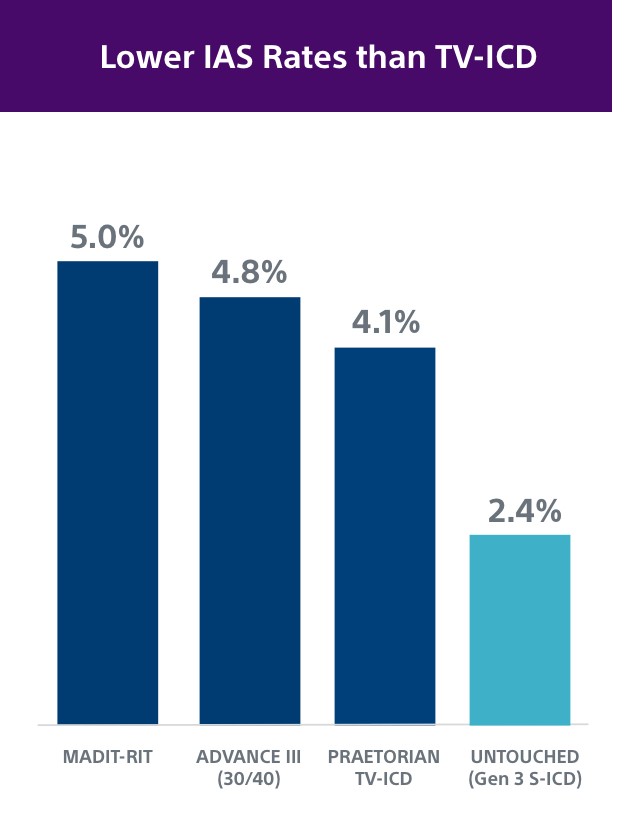
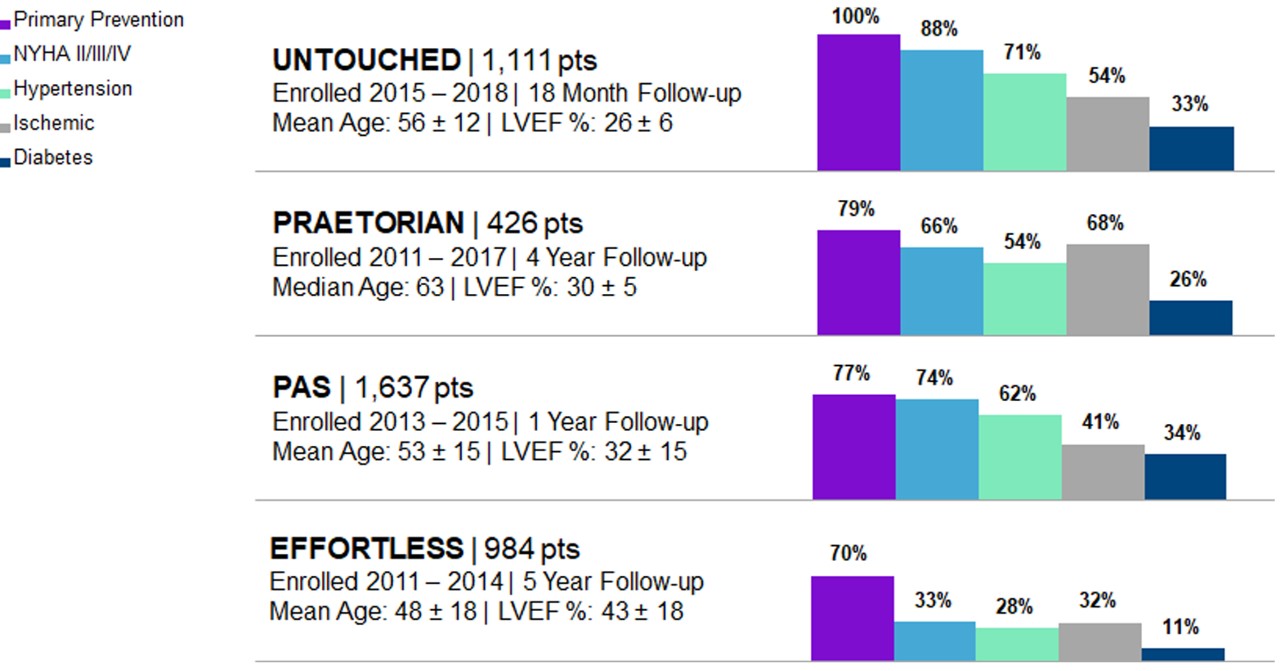
As S-ICD Technology Evolves, So Does the Clinical Data
Early S-ICD trials typically had younger patients with less advanced heart disease and “niche” indications, including channelopathies, hypertrophic cardiomyopathy, congenital heart disease or previous ICD indication. However, both the PRAETORIAN and UNTOUCHED studies included older and sicker patients. In fact, UNTOUCHED included the most traditional cohort of patients (primary prevention, LVEF ≤ 35%) and showed the S-ICD has lower inappropriate shock (IAS) rates than TV-ICDs.
Patient Comorbidities and S-ICD
It’s important to consider patient comorbidities and other risk factors for complications when determining whether a TV-ICD is required or if a patient should be offered both S-ICD and TV-ICD when taking a shared decision-making approach to the treatment decision.
Patient Comorbidities |
S-ICD |
TV-ICD Required2,8 |
TV-ICD Considered2,8 |
|
|---|---|---|---|---|
| Evaluating Need for Brady Pacing7,23-24 | Brady pacing indication at implant |
|
|
|
No current pacing indication, but has 1 or more of the following:
|
|
|
||
| No pacing indication at implant and age < 80 |
|
|
|
|
| High Risk for TV Lead Failure25 | Life expectancy > 8 years |
|
|
|
| High Risk for Infection15 | H/O device infection |
|
|
|
| Prosthetic heart valve |
|
|
||
| On dialysis or renal insufficiency |
|
|
||
| Diabetes |
|
|
||
Other risk factors:
|
|
|
||
| High or Low Risk for ATP26-27 | Ischemic or non-ischemic heart failure or ICD-indicated patient with NO history of recurrent sustained monomorphic VT |
|
||
ICD-indicated patient WITH a history of recurrent sustained monomorphic VT amenable to ATP therapy |
|

Education & Training

Discover the Next Evolution in S-ICD Therapy
The EMBLEM™ MRI S-ICD System protects patients at risk of sudden cardiac death (SCD), while minimising complications linked to transvenous or substernal leads.