")

")
")


")
")




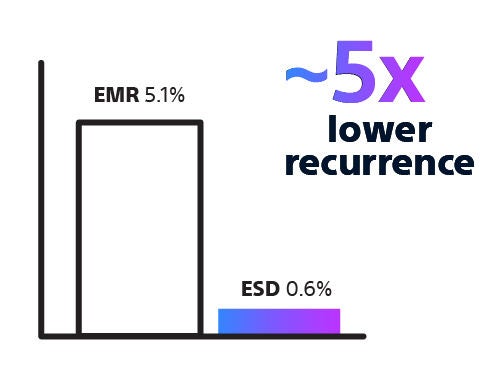
Endoscopic resection techniques are used to remove superficial gastrointestinal lesions using minimally invasive approaches. The primary techniques include EMR, ESD, and hybrid techniques, each selected based on lesion characteristics and procedural complexity.
Choosing the Right Approach
Endoscopic resection presents procedural challenges, particularly when lesion size, morphology, and location vary. These factors, along with operator expertise, can increase procedural complexity, influence workflow, and affect the likelihood of complete resection and the need for additional interventions.
Successful resection begins with selecting an approach that matches lesion characteristics and procedural intent. Reliable resection technologies that support precise tissue capture and controlled dissection can help you manage complexity, perform consistently across a range of scenarios, and enable effective, organ-preserving treatment when clinically appropriate.
Clinical Workflow

Our clinical workflow moves from lesion detection through technique selection (EMR, ESD, or Hybrid), to resection, and closure where required.