
")

")

")
")


")
")




Direct Endoscopic Visualization via Cholangioscopy Before and After Radiofrequency Ablation
Biliary Decompression of Strictures for Patient with Cholangiocarcinoma
 Bret Spier, M.D.
Bret Spier, M.D.Gastroenterology
IU Health
Bloomington, IN
Patient History
Procedure

Figure 1

Figure 2
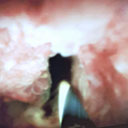
Figure 3

Figure 4
Outcome
Conclusion
Educare
To explore in-depth physician-led lectures, procedural techniques and device tutorials, visit Educare.
Get started