


")

")
")


")
")



Complex stone case: John
Discover how our solutions can assist you in managing patients with complex or difficult biliary stones.
Start of symptoms

John, a 52-year-old male, presented at the emergency department due to persistent and intense pain in the right upper quadrant that had persisted for more than a week. Additionally, blood tests demonstrated abnormal liver enzyme levels.
A magnetic resonance cholangiopancreatography (MRCP) was conducted, revealing the following findings:
- A 25 mm filling defect located in the distal common bile duct.
- Dilatation observed in the upstream sections of the common bile duct (CBD), common hepatic ducts, and intrahepatic bile ducts.
- Distension of the gallbladder.
Following the MRCP findings, John underwent an Endoscopic Retrograde Cholangiopancreatography (ERCP), which revealed:
- A significant oval-shaped stone, measuring 2.8 cm, located in the distal common bile duct (CBD).
- Additionally, multiple smaller filling defects were observed.
John’s treatment
1. Initial ERCP & Balloon Sphincteroplasty
The physician initiated the treatment process for extracting the CBD stone with an endoscopic sphincterotomy, followed by a large balloon sphincteroplasty (up to 15 mm), and dilation-assisted extraction using a CRETM RX Biliary Balloon Dilation Catheter. However, these methods alone were not suitable for removing the large stone.
Procedure steps included:
Endoscopic sphincterotomy
Large balloon sphincteroplasty (up to 15 mm)
Stone extraction balloon
However, at this stage, the stone could not be retrieved.
The ESGE recommends limited sphincterotomy combined with endoscopic papillary large-balloon dilation as a first line approach to remove difficult common bile duct stones. Strong recommendation, high quality evidence.5
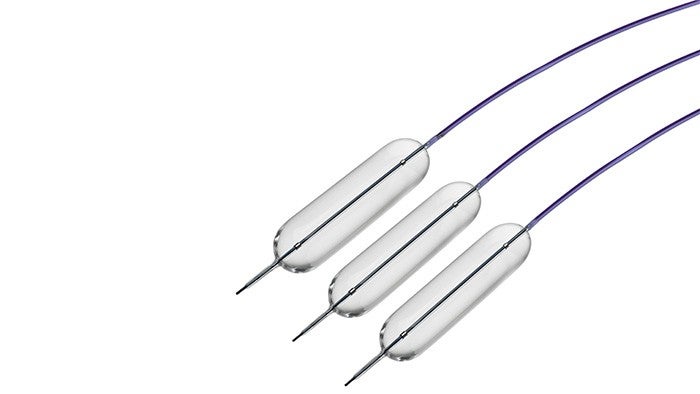
CRE™ Balloon Dilatation Catheter
The CRE™ RX Biliary Balloon Dilatation Catheter is indicated for use in adults for endoscopic dilatation of the sphincter of Oddi with or without prior sphincterotomy.
The CRE™ RX Biliary Balloon Dilatation Catheters may also be used for injection of contrast medium for fluoroscopic visualization of the bile ducts.
2. Cholangioscopy
Given the large size of the biliary stone and the challenges encountered in removing it during the initial ERCP procedure, the clinician categorised this as a difficult bile duct stone due to its size and the narrow anatomy of the distal common bile duct. Consequently, the decision was made to use the SpyGlass™ DS Direct Visualization System, a single-use cholangioscope, for further evaluation and management.
SpyGlass™ DS Direct Visualization System
In the context of ERCP, patients may benefit from direct visualization as it may enable more efficient clinical evaluations compared to traditional ERCP.

3. Fragmentation with EHL
After accessing the bile duct with SpyGlass, the physician successfully visualized the sizable stone and opted to employ the Autolith™ Touch Biliary EHL System to break down the stone. The procedure was aided by the SpyGlass™ DS for direct visualization.
The ESGE recommends the use of cholangioscopy assisted intraluminal lithotripsy as an effective and safe treatment of difficult bile ducts.
Autolith™ Touch Biliary EHL System
Designed for ease and efficiency, EHL represents a safe and effective technique to achieve stone clearance in complex cases, by using shockwaves to fragment stones.3

4. Stone Extraction with ExtractorTM Pro RX-S Retrieval Balloon
SpyGlass™ cholangioscopy was repeated after fragmenting the distal bile duct stone and clearing the fragments utilising the Extractor™ Pro RX-S Retrieval Balloon.
Following the fragmentation of the distal bile duct stone using AutoLith, the stone fragments were extracted by trawling the bile duct using the Extractor™ Pro RX-S Retrieval Balloon.
The SpyGlass was reintroduced to conduct further visual examination of the bile duct, revealing another sizable stone impacted at the cystic duct, partially obstructing the bile duct lumen. This condition corresponds to Type IV Mirizzi syndrome according to the Csendes classification.
Extractor™ Pro RX-S Retrieval Balloon
Can help facilitate effective and efficient stone removal.

5. Mirrizzi Stone Fragmentation EHL
The impacted stone within the cystic duct went unnoticed in the initial MRCP examination. However, it was successfully identified through SpyGlass and direct visualization, allowing for complete fragmentation using EHL.
Managing CBD stones with balloon or basket catheters can be challenging due to specific stone features, their location, the anatomical characteristics of the biliary tract, or the patient’s clinical needs. In such cases, a combined approach of direct visualisation and a powerful, precise fragmentation may enable optimal outcomes.
6. Stone Extraction
To address the remaining stone fragment, the clinician utilised the ExtractorTM Pro RX-S Retrieval Balloon successfully eliminating the residual stone fragments.
In a recent study, 15/50 patients (30%) were found to have residual biliary stones that were not seen by occlusion cholangiography but were detected when the SpyGlass™ DS System was used.4
Extractor™ Pro RX-S Retrieval Balloon
Use of this device allowed stone fragments to be removed.

7. Residual Stone fragment removal SpyGlassTM Retrieval Basket
A final inspection using the SpyGlass™ DS revealed small remaining fragments, which were subsequently extracted using the SpyGlassTM Retrieval Basket. This comprehensive approach led to the complete restoration of both the bile duct and cystic duct, ensuring their patency.
SpyGlass™ Retrieval Basket
This device can be used to capture and remove residual biliary and pancreatic stones and stone fragments visualised with the SpyGlass™ DS System.

Bringing to an end John’s discomfort

After the successful procedure, John witnessed a remarkable improvement in his symptoms, prompting his discharge from the hospital the next day. Finally finding relief from his discomfort, he conveyed deep gratitude to his medical team for their exceptional expertise and compassionate care.