
")

")

")
")


")
")




Repeat Radiofrequency Ablation Treatment Combined with Stone Lithotripsy to Maintain Biliary Drainage
 Rajeev Nayar, M.D.
Rajeev Nayar, M.D.Advanced Gastroenterologist
AMITA Health
Chicago, IL
Patient History
Procedure
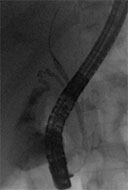
Figure 1
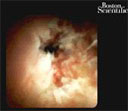
Figure 2

Figure 3
Outcome
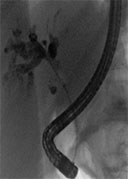
Figure 4
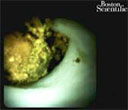
Figure 5
Conclusion
More Case Studies
Treating Pancreatic Necrosis using the 20mm AXIOS™ Stent & Electrocautery Enhanced Delivery System
Fragmenting and Removing a Complex Biliary Stone under Direct Visualization
Educare
To explore in-depth physician-led lectures, procedural techniques and device tutorials, visit Educare.
Get started