")

")

")
")


")
")



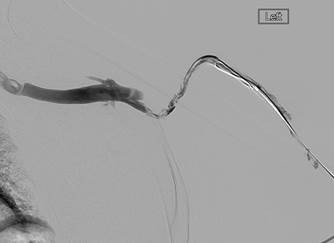
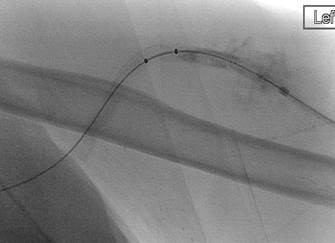
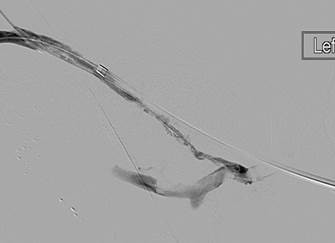
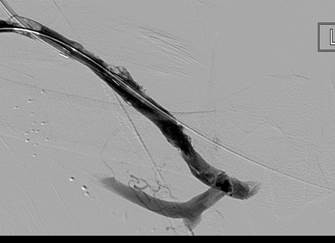
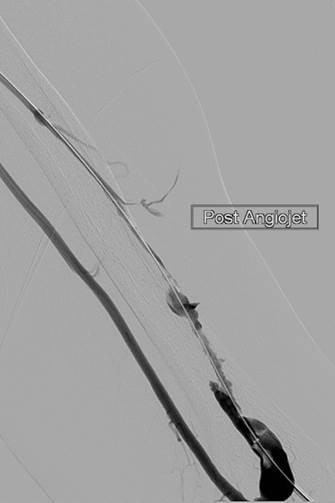
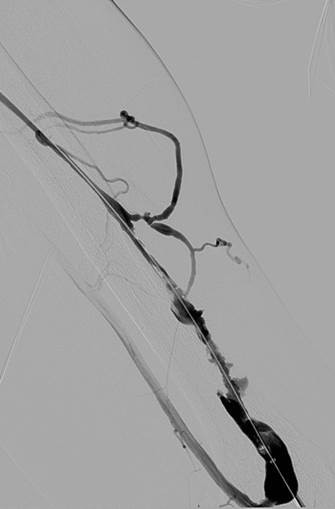
AngioJet™
Ultra Thrombectomy System
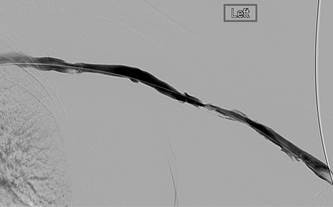
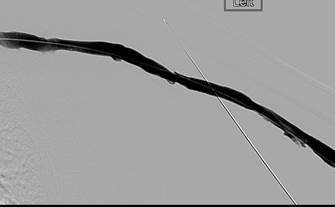
Thrombectomy of left brachiocephalic AV fistula
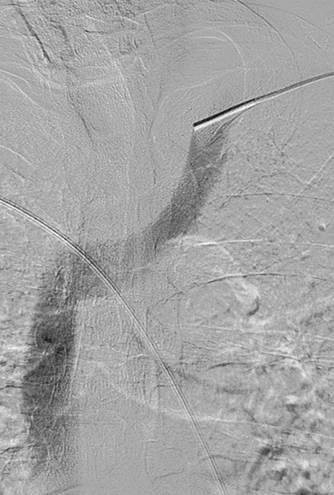
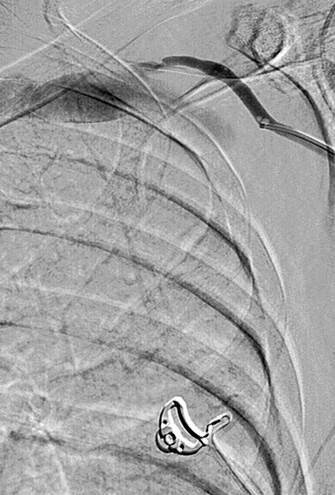
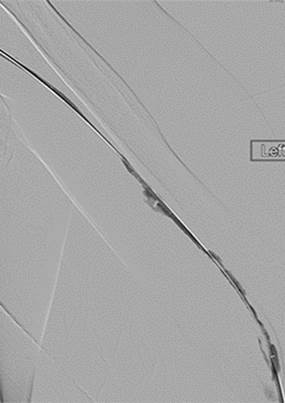
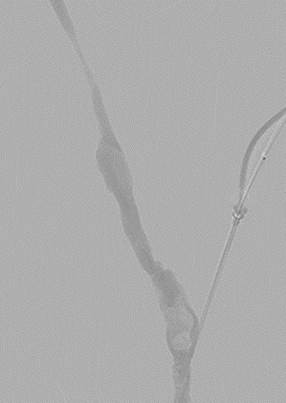



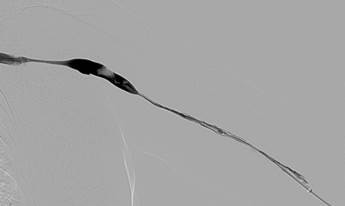
Dr. R. Jones, Interventional Radiologist, Queen Elizabeth Hospital Birmingham, UK.
Thrombectomy of occlusion of left brachiocephalic fistula
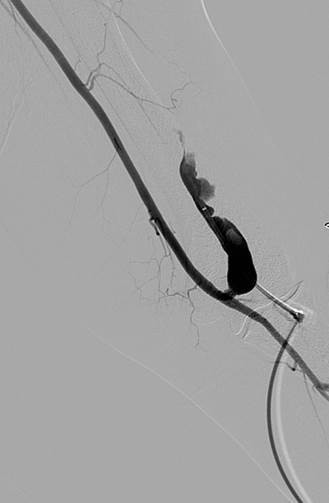
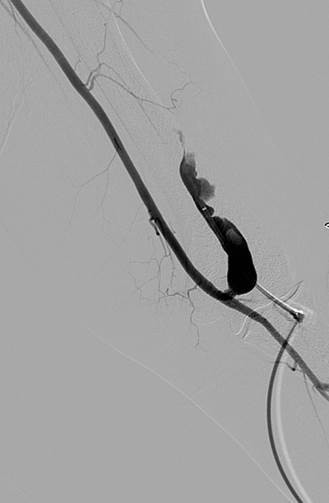

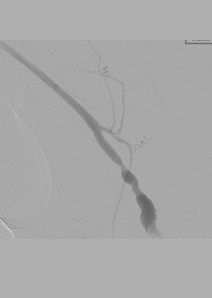
Thrombectomy of left brachial artery-axillary vein graft