
")

")

")
")


")
")



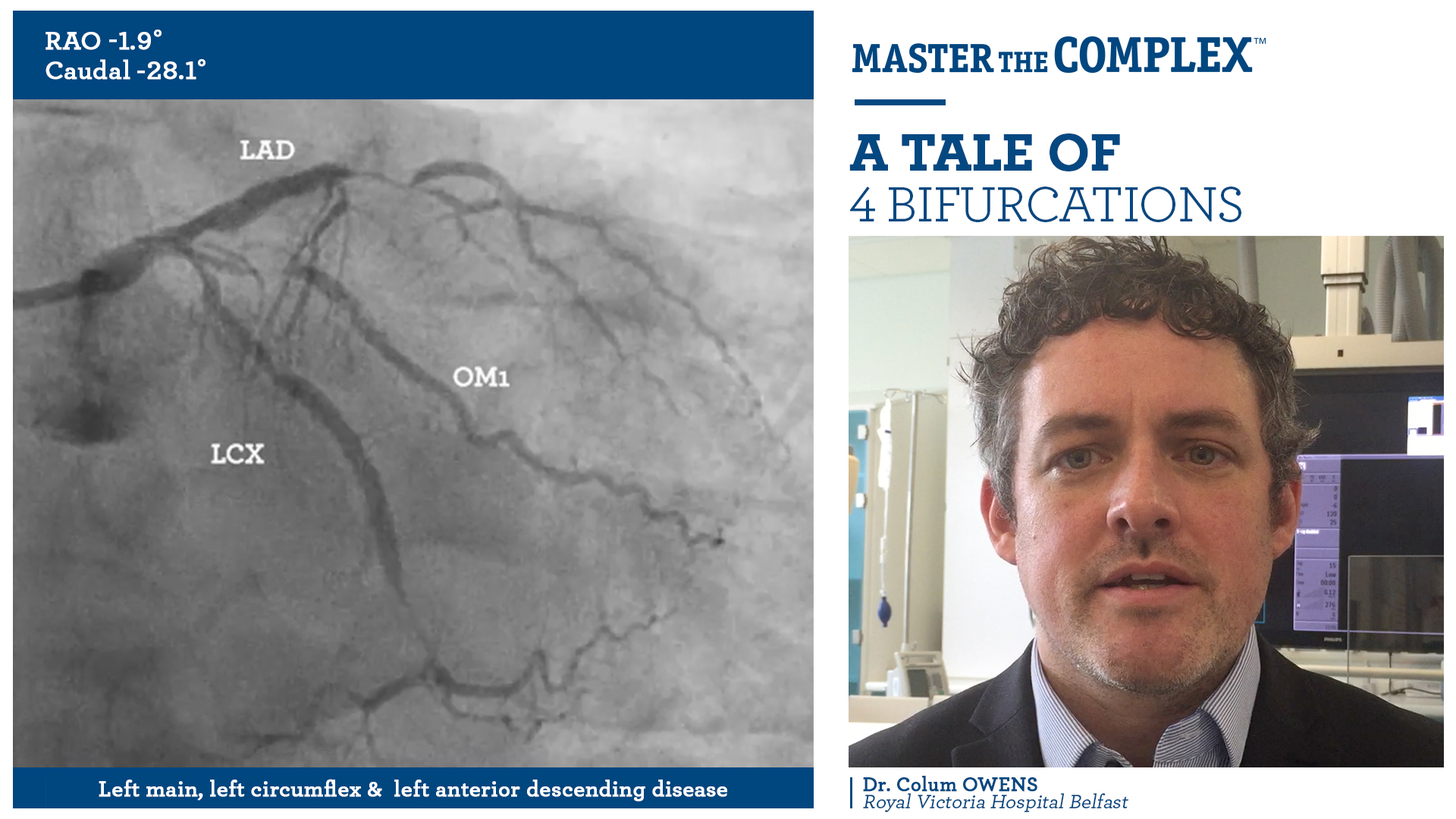
Case Study: A Tale of 4 Bifurcations
Key learnings
 | Interventional strategies to deal with complex bifurcation disease in a patient presenting with cardiogenic shock. |
|---|---|
| How a robust knowledge of stent characteristics allow for full revascularisation in patients with complex disease |
| The importance of stent choice where DAPT duration considerations are important |
Patient History
- 57 year old male. Ex-smoker. 1st presentation of ischemic heart disease
- Presented with a one week history of progressive angina and an anterolateral ST-elevation myocardial infarct complicated by cardiogenic shock
Clinical Presentation
- Unwell on arrival with blood pressure of 78/42 mmHg
- Echo: severe LV dysfunction with LVEF of 30%
- Right radial access, 7Fr sheath
- Diagnostic angiography showed severe 3-vessel disease with complex bifurcations involving the distal right coronary artery (RCA) (Watch Distal RCA Angio), left main stem (LMS) , left circumflex bifurcation (LCX) (Watch Left Main Angio) and an occluded left anterior descending/2nd diagonal artery bifurcation (LAD/D2) (Watch Occluded Left Angio)
- After surgical discussion, decision taken to re-vascularise with percutaneous revascularisation



Techniques Used
- Primary PCI
- Multiple complex bifurcation techniques including modified crush, mini crush and culotte with use of anchoring balloons
SYNERGY Platform characteristics
- The two connector design on the stent body, vessel conformability4 and large side-branch access3 allowed for multiple bifurcation techniques
- Ability of stent overexpansion, when called for during post dilatation, to match the diameter of larger vessels, and permits complex LM intervention. (The SYNERGY 4.0 mm dedicated stent has a labeled overexpansion capability of up to 5.75 mm5)
- Its deliverability, visibility and conformability4 allowed for full revascularisation of complex disease
SYNERGY Drug & polymer characteristics
- Abluminal coating and synergistic drug release1 with polymer degradation* facilitates early healing6 from day one and thus allows for flexibility of DAPT duration7. Polymer is gone after completion of drug elution at 3 months. This is an important consideration when baseline morbidity is unknown as in this case where the patient presents with cardiogenic shock
Acute Procedure (Primary PCI to LAD/D2 bifurcation)
- Flow re-established in LAD/D2 with a 2.5 mm compliant balloon but D2 dissected
- A “crush” bifurcation strategy chosen for 2 reasons: vessel size disparity and maintaining flow in dissected diagonal by stenting it first with a 2.25 x 32 mm SYNERGY DES placed from mid LAD to D2 and optimised with a 2.5 mm NC EMERGE balloon
- Crushed with 3.0 x 15 mm compliant balloon in LAD (modified crush technique – using a balloon rather than a stent)
- LAD then stented with 3.0 x 32 mm SYNERGY DES optimising with a 3.5 NC EMERGE balloon
- Final kissing balloon inflation in LAD/D2 with 3.5 and 2.5 mm NC EMERGE balloon respectively with TIMI III flow restored

Acute Procedure (Left main/circumflex bifurcation)
- Complex residual disease involving LM, proximal LAD and LCX
- Second marginal circumflex (OM2) directly stented with a 2.25 x 24 mm SYNERGY DES optimising with a 2.5 mm NC EMERGE balloon
- 1st marginal circumflex (OM1) stented directly with a 2.5 x 24 mm SYNERGY DES back into left main/LCX os in a “mini crush” strategy, optimised with a 3.0 mm NC balloon and crushed with a 3.5 mm balloon in the LMS
- LMS to LAD stented with a 4.0 x 28 mm SYNERGY DES and optimised with a 4.0 mm NC balloon. The LMS was proximally optimised with a 5.0 mm NC balloon ensuring both stent apposition and side branch access to the LCX, and demonstrating stent over-expansion characteristics
- Final kissing balloon inflation in LMS/OM1 bifurcation with 4.0 and 3.0 mm NC balloons resulting in resolved cardiogenic shock and improved ST segments


Elective Procedure (Distal RCA bifurcation-Culotte)
- Residual disease addressed in order to complete revascularisation
- Distal RCA bifurcation treated using culotte technique as branches comparable in size
- PLB stented with a 2.5 x 28 mm SYNERGY DES, optimising with a 3.0 and 3.5 mm NC EMERGE balloon
- Distal RCA stented into the PDA with a 2.5 x 24 mm SYNERGY DES and optimised with a 3.0 mm NC EMERGE balloon
- Distal RCA to PL bifurcation culotted with a 3.0 x 38 mm and a 4.0 x 20 mm SYNERGY DES in an overlapping fashion, optimising with 3.5 and 4.0 mm NC EMERGE balloons
- Final kissing balloon inflation into PL/PDA bifurcation with 3.5 and 3.0 NC EMERGE balloons respectively

OM1/OM2 bifurcation (Culotte)
- Check angiogram showed patent stents but significant residual OM2/OM1 bifurcation disease
- To address this complex residual bifurcation disease, a 7Fr guide and anchoring balloon technique was used in OM1 to facilitate stent delivery in OM2
- Using a 2.5 mm EMERGE in the OM1for anchoring a 2.5 x 24 mm SYNERGY DES was delivered into the OM2 and optimised with a 3.0 mm NC EMERGE balloon to high pressure in a culotte technique
- A final kissing balloon inflation undertaken in the OM1/OM2 bifurcation with a 2.5 and 3.0 mm NC EMERGE balloon respectively
- The LMS/OM2 bifurcation finally optimised with a kissing balloon inflation 5.0 and 3.0 mm NC EMERGE balloons respectively with excellent final result


1 Eppihimer M, PhD. Impact of Polymer Type and Location on Stent Thrombogenicity and Endothelial Cell Coverage. EuroPCR 2014
2 Chen YL, PhD, Foss A, PhD, Eppihimer M, PhD, et al. Characterization of In Vivo Poly(DL-lactic-co-glycolic acid) Bioabsorption from a Drug-Eluting Stent. EuroPCR 2012
3 Stent_MECD_Technical _Report; PDM doc.91019938
4 Data on file at Boston Scientific. Bench testing performed by Boston Scientific Corporation. Bench test results not necessarily indicative of clinical performance
5 SYNERGY Stent Systems DFU
6 SORT OUT VIII presentation by Ida Riise Balleby, MD at PCR 2015; 2 month OCT Analysis presentation by J. M. de la Torre, MD at TCT 2014; TIMELESS presentation by Juan Granada, MD, at CRT 2015; Burgos-Santander study presentation by J. M. de la Torre, MD at PCR 2015
7 SYNERGY is designed with a low initial polymer load, abluminal coating and bioabsorbable polymer which may reduce the risk of thrombosis and the need for prolonged dual antiplatelet therapy. In selected higher risk patients where the physician determines that the risks outweigh the benefits of continued DAPT, it may be reasonable to interrupt or discontinue therapy after 1 month based on low stent thrombosis rates and no observed increased risk for stent thrombosis as shown in the current literature.