
")

")

")
")


")
")




2021 Congress season is coming to the end, that’s why we would like to share with you the last findings on HeartLogic presented at one of the most important international meetings: the Heart Failure Society of America Congress.
In the Late Breaking Clinical Trials session, the Multiple Cardiac Sensors presented an HeartLogic analysis for the Management of Heart Failure (MANAGE-HF) study: a trial designed to evaluate the clinical efficacy and usefulness of HeartLogic. Moreover, in the Poster Session has been presented an interesting analysis about the use of HeartLogic as “COVID Index”.
As usual, in this newsletter you can find also an interesting case of the month.
Heart Failure Society
of America Congress 2021

Late Breaking Clinical Trials
The last findings about the MANAGE-HF Trial have been presented by Dr. Allen during the Late Breaking Clinical Trials session.
Variation in Treatment Responses to HeartLogic Heart Failure Alerts in the Multiple Cardiac Sensors for Management of Heart Failure (MANAGE-HF) Study
The Multiple Cardiac Sensors for Management of Heart Failure (MANAGE-HF) study was designed to evaluate whether the HeartLogic algorithm can be integrated into care and improve outcomes. In the Phase 1, the actual treatment responses to alerts and their association with heart failure events have been reported and analyzed.
This sub-analysis enrolled 200 patients, 31 of them from US and Europe, implanted with CRT-D or ICD devices equipped with HeartLogic algorithm and who had a hospitalization for heart failure within 12 months or an unscheduled visit for heart failure exacerbation within 90 days.
Methods:
Sites were required to initiate a qualified treatment (over the phone ore through in-office visit) within 7 days after HeartLogic threshold crossing.
- Enforce adherence if suboptimal
- Change current heart failure medications to address signs and symptoms
- Treat other conditions (e.g., new AF, uncontrolled DM)
A treatment response score (0-2) was created based on the frequency and type of response to alerts in order to quantify variability in responses to HeartLogic alerts. Weekly alert treatment score was assigned as follows:
- 2 points > augmentation of a decongestive medication (loop diuretics, thiazide, ARNI, vasodilators)
- 1 point > augmentation of a beta-blocker, ACEI, ARB, or MRA
- 0 points > otherwise
Results:
During a mean follow-up of 20.9 ± 7.5 months 585 HeartLogic alerts occurred and 74% of cases required Heart Failure medication increase, for a total of 1766 changes in Heart Failure medication.
The alerts were followed, in the next 30 days, by:
- 76 heart failure Hospitalizations (primary reason for admission)
- 19 Hospitalizations (heart failure as secondary reason for admission)
- 23 intravenous outpatient treatments
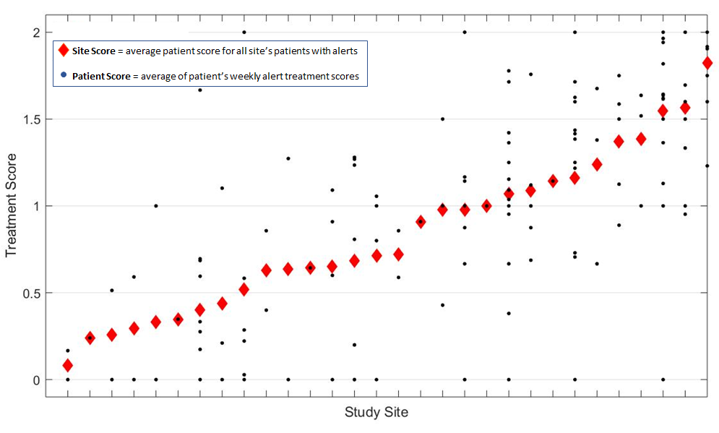
The Figure 1 shows the average patient score for each site: it results that treatment scores across sites and patients were highly variable.
The analysis reported also a marked variability in treatment type across sites: changes only in diuretic drugs, diuretic and non-diuretic Heart Failure medications or only non-diuretic Heart Failure medications.
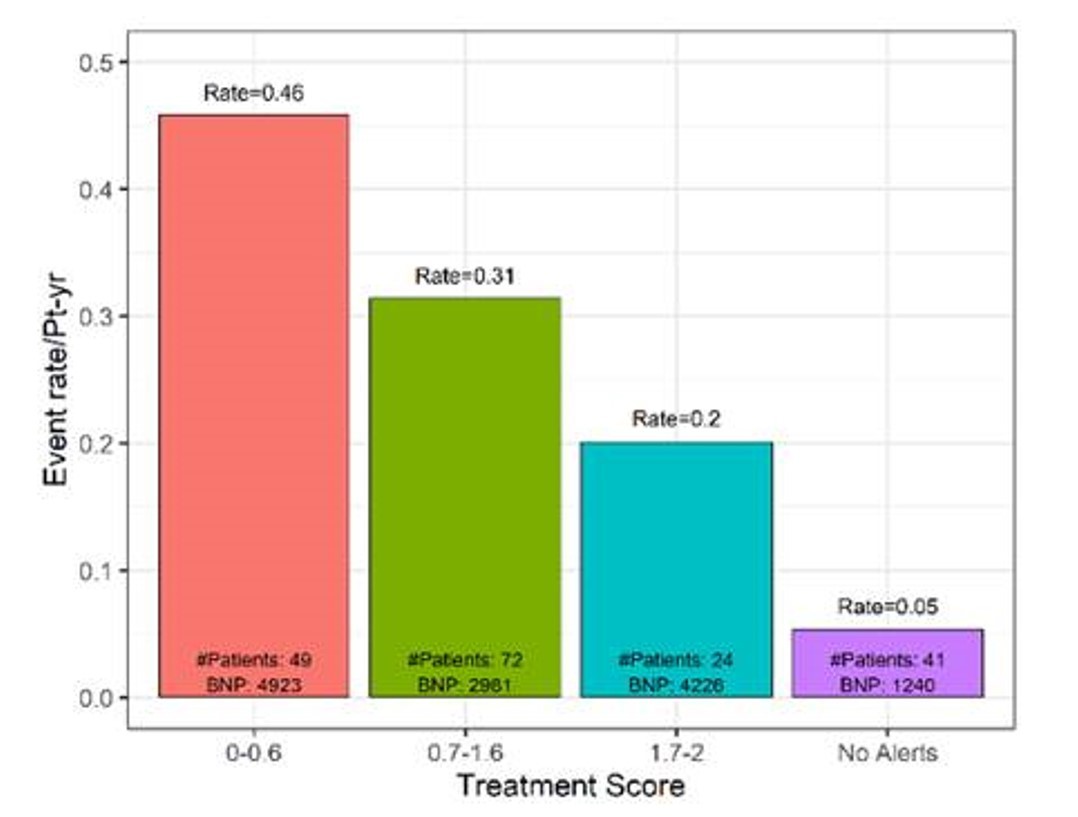
The association between patient treatment score and heart failure event rate showed that there was a trend for fewer heart failure events when more consistent heart failure treatment was given in response to alerts.HeartLogic index recovered faster when decongestive HF treatment were provided in response to the alert.
Moreover, this analysis confirms that patients with HeartLogic alerts have higher risk of heart failure events: the average HF event rate for patient with HeartLogic alerts was 0.35 events/pt-yr, while for patients without HeartLogic alerts was 0,05 events/pt-yr.
Conclusion:
- Heart failure treatment in response to HeartLogic alerts was variable across patients and sites
- The analysis showed a trend towards fewer heart failure events associated with more marked heart failure treatment provided in response to the alerts
- There was a quicker resolution of HeartLogic alerts when decongestive treatment was given in response to the alert.
Poster Session

This poster presented by Dr. Panta analyzed two heart failure patients implanted with CRT-D devices equipped with HeartLogic algorithm and diagnosed positive for COVID-19 infection.
The objective of the analysis was to assess if HeartLogic can be used as a functional tool to early detect COVID-19 , monitor heart Failure status and predict the severity of COVID-19 symptoms in patients with advanced heart failure.
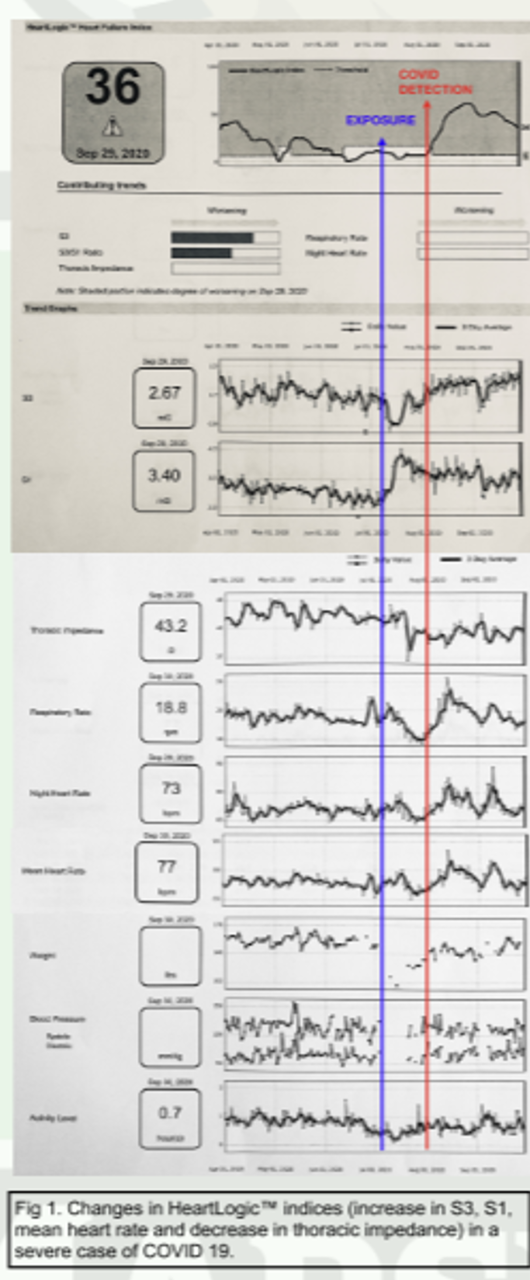
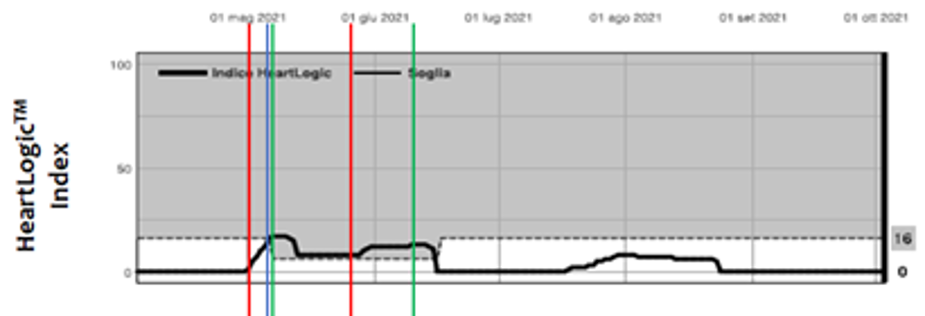
A 83-year–old man with history of non-ischemic cardiomyopathy, persistent atrial fibrillation underwent implantation of a CRT-D device and was being monitored with HeartLogic for two years.
One week prior to hospital admission HeartLogic index identified changes. The cardiology team promptly evaluated causes: patient reported dry cough, intermittent rhinorrhea, dyspnea and he tested positive for COVID-19 (red line). The BNP value was very high (18.000 pg/ml) and the patient was admitted to hospital, intubated and mechanically ventilated for impending respiratory failure. After few days he was successfully extubated without major complications.
He continued to improve clinically and was discharged while the HeartLogic index started to decline with return to baseline values.
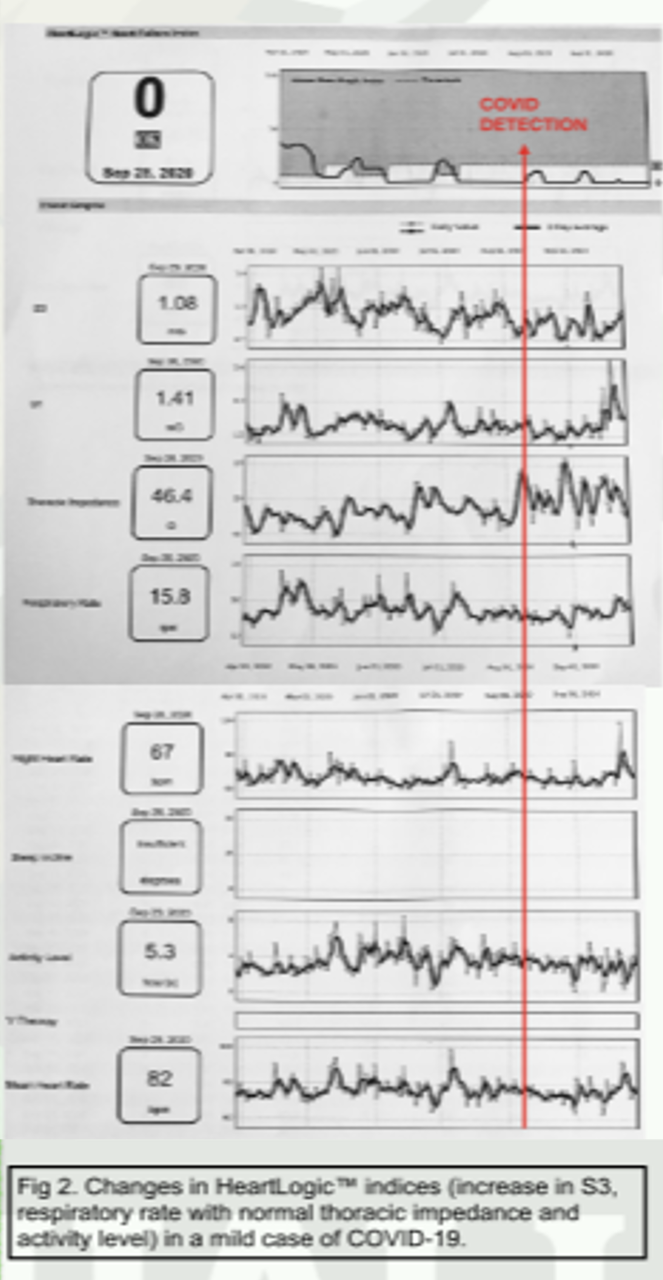
A 59-year-old man with ischemic cardiomyopathy and CRT-D implantation, recurrent admissions for heart failure and awaiting heart transplant, was diagnosed positive for COVID-19 infection.
He developed a minor cough, hoarseness, generalized weakness and light headedness. Abdominal pain wit nausea and vomiting, but no signs or symptoms of heart failure (orthopnea, nocturnal dyspnea, edema, weight gain,...) or BNP increase were reported.
During infection, the HeartLogic index remained stable and didn’t cross the threshold, as no impending heart failure event was detected.
Patient recovered from Covid-19 without any major clinical events.
In the first case HeartLogic helped making early diagnosis of COVID-related heart failure (allowing early treatment and improving outcome), while in the second case the algorithm allowed to monitor the symptoms and predicted a milder impact.
Conclusion:
HeartLogic index could serve as a “COVID-19 index” to early diagnose infection. Indeed, it correlates with the severity of symptoms and predicts the outcome in advanced heart failure patients diagnosed with COVID-19.
The index could also provide the cardiology team more time to adjust and optimize treatment, improve outcome and adopt a proactive care rather then reactive treatment.
Case of the month
A 67-year old man with hypertension, family history of ischemic heart disease, COPD and implanted with CRT-D device in 2013, underwent a LVAD implantation in February 2020. Some months later, on October 9th, 2020, the patient underwent the defibrillator replacement with a Vigilant X4 CRT-D device. Then, the Latitude remote monitoring system and HeartLogic algorithm were activated.
From February to May 2021…