
")

")

")
")


")
")




After the summer break, we are ready to start again our monthly appointment. We are delighted to share with you an interesting analysis on HeartLogic which has been recently published on Circulation Heart Failure Journal. Also, we are pleased to present you an overview of the HeartLogic abstracts displayed at ESC Congress 2021.
In this issue you can also find a new case of the month.
HeartLogic and Risk Stratification
An interesting analysis about the heart failure risk stratification with HeartLogic carried out by Prof. Calò et al has been published on the Circulation Heart Failure Journal (Circulation: Heart Failure. 2021):
Multiparametric Implantable Cardioverter-Defibrillator Algorithm for Heart Failure Risk Stratification and ManagementAn Analysis in Clinical Practice
A previous subanalysis of the MultiSENSE Study showed the value of HeartLogic as a measure of the risk of heart failure events, independent from baseline clinical variables1.
The analysis published by Calò et al. evaluated:
- the risk stratification ability of the algorithm in clinical practice in patients who received HeartLogic-enabled ICDs and CRT-Ds.
- the management strategies adopted in response to the alert and their association with the occurrence of heart failure events.
The analysis was performed in clinical practice: remote data reviews and patient phone contacts were taken in response to HeartLogic alert and physicians were free to implement clinical actions they considered appropriate (remotely or in-office).
The HeartLogic feature was activated in 366 ICD and CRT-D patients at 22 centers and during a median follow-up of 11 months [25th–75th percentile: 6–16] 273 HeartLogic alerts occurred (0.76 alerts/patient-year) in 150 patients. The total time IN the alert state was 11% of the total observation period.
HeartLogic Alerts and Heart Failure Events
The rate of heart failure hospitalization or death was 0.12/patient-year during observation period: 36 HF hospitalization in 21 patients and 8 HF deaths.
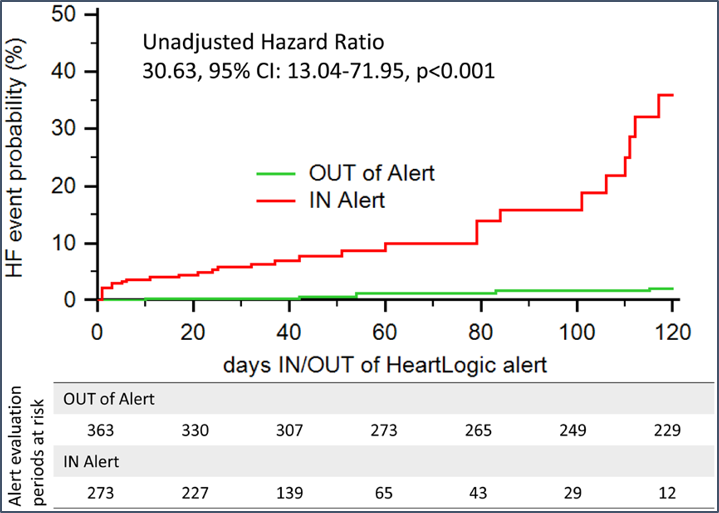
- 35 events occurred in the HeartLogic IN alert state (an event rate of 0.92/patient-year);
- 9 events occurred in the HeartLogic OUT of alert state (a rate of 0.03/patient-year).
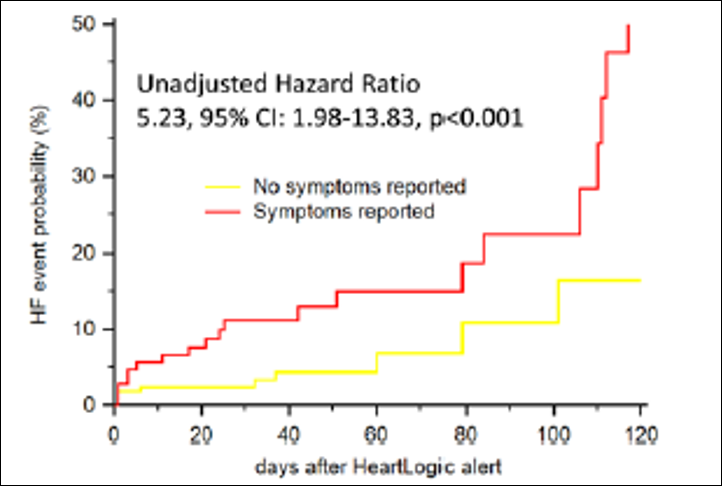
Comparison of the event rate in the IN alert state with that in the OUT of alert state yielded a hazard ratio (HR) of 30.63 (Figure 1).
Alert Management and Association With Heart Failure Events
A total of 273 HeartLogic alerts occurred during the observation period and the study evaluated the alerts outcomes according three different management aspects.
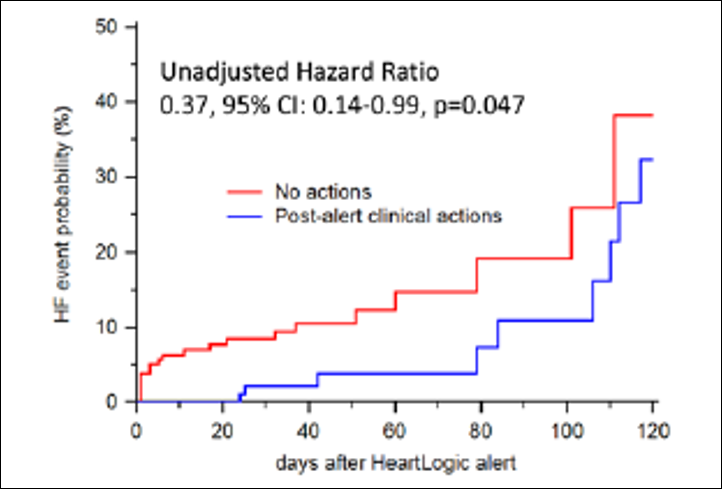
- Clinical actions: 117 (43%) alerts triggered clinical actions in response to them.
The most frequent actions undertaken to manage the heart failure conditions detected by the HeartLogtic alerts were (multiple actions per alert):
- 66% diuretic dosage increase;
- 34% other drug adjustment;
- 6% patient education on therapy adherence;
- 3% device reprogramming.
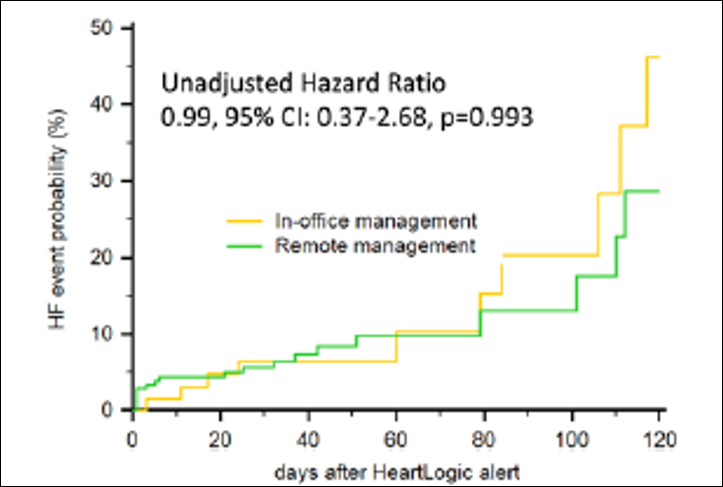
- Remote/in-office management: 204 (75%) alerts were managed remotely.
- HF symptoms: 107 (39%) alerts were associated with symptoms of HF worsening at the time of the first remote examination.
The most frequent symptoms reported were (multiple symptoms per event):
- worsening of dyspnea on effort or at rest in 93 (87%) cases;
- fatigue in 65 (61%) cases;
- orthopnea in 22 (21%) cases.
Conclusions:
- HeartLogic is able to identify patients during periods of significantly increased risk of heart failure events.
The use of HeartLogic may enable an efficient use of healthcare resources for the management of patients with HF (the time IN alert state is much shorter than that of OUT of alert state periods).
- When clinical actions are undertaken in response to alerts, the rate of heart failure events seems lower
The rate of alerts is low, and this would not generate a high workload at the centers in case an alert based management strategy was adopted.
- The absence of an in-office visit after a HeartLogic alert did not impair the patient’s outcome
HeartLogic alerts may be safely managed remotely, without increasing the workload of the clinic.
- The presence of symptoms at the time of HeartLogic alert was associated with a higher risk of heart failure events
Verification of symptoms seemed useful to better stratify patients at risk of HF events.
ESC 2021 Congress
The ESC Congress took place from 27 to 30 August 2021.
During the event the latest clinical updates and the new ESC Clinical Practice Guidelines for Heart Failure were shared.
Two interesting posters about HeartLogic performance were presented:
- the first one from the Spanish RE-HEART registry;
- the second one from an Italian center, which describes their experience during COVID-19 pandemic.
Poster Session

The poster, presented by Dr. De Juan Baguda, analyzes the association between HeartLogic alerts and clinical events, describing the implementation of the algorithm for remote heart failure patients management in clinical practice.
RE-HEART registry was divided in three phases:
- Phase 1: physicians were blinded to the HeartLogic alert status;
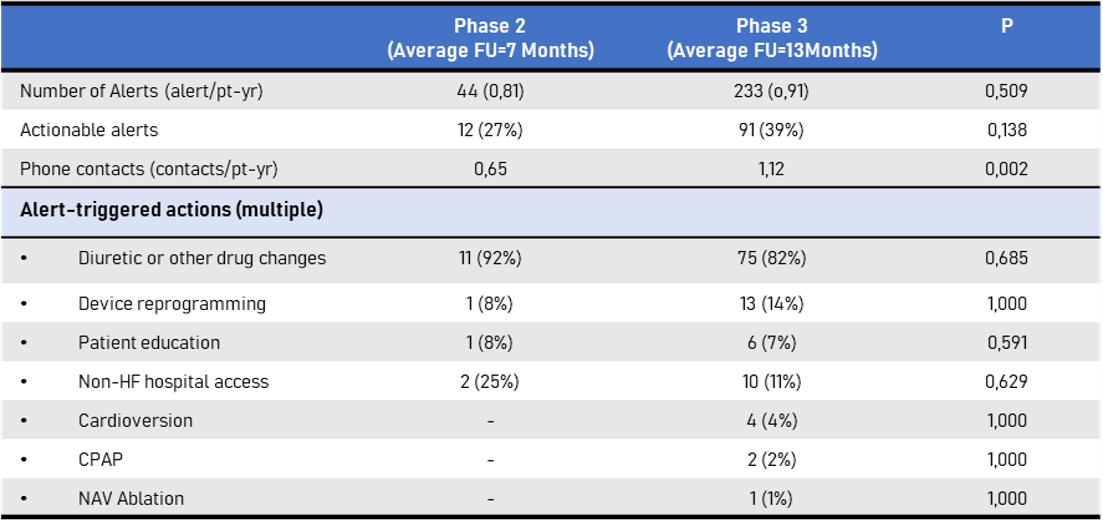
- Phase 2: physicians reacted to HeartLogic alerts according to their clinical practice;
- Phase 3: physicians followed a standardized protocol in response to HeartLogic alerts.
The registry enrolled 288 patients who received HeartLogic-enabled ICD or CRT-D at 15 Spanish centers.
Blinded Phase (Phase 1): 101 patients
During a median observation period of 10 months, the HeartLogic index crossed the alert-threshold value 73 times in 39 patients: 0.72 alerts/patient-year.
During HeartLogic in alert status:
- 8 heart failure hospitalizations and 2 emergency rooms admissions occurred in 9 patients: 0.10 events/patient-year;
- 10 minor events (heart failure in-office visits and non-heart failure hospitalizations).
Active Phases (Phases 2 and 3): 267 patients
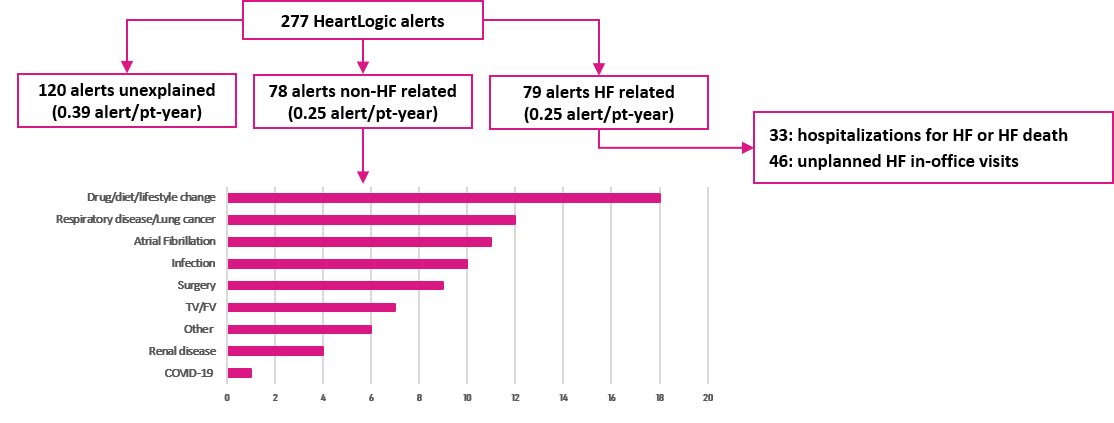
During a follow-up of 16 months, the HeartLogic index crossed the alert-threshold value 277 times in 136 patients: 0.89 alerts/patient-year.
Conclusions:
- HeartLogic index was frequently associated with heart failure-related clinical events, with a low rate of unexplained events.
- The HeartLogic alert and a standardize protocol of actions allowed to remotely detect impending decompensation events and to implement clinical actions with a low workload for the centers.

This poster, presented by Dr. Amellone from Turin Hospital, was a single Italian center experience to evaluate the HeartLogic performance in detection of heart failure events during the Covid-19 pandemic.
Heart failure patients with HeartLogic-enabled CRT-D devices were enrolled in the study.Remote data were reviewed every month and at the time of HeartLogic alert. In case of HeartLogic alerts, patients were contacted by phone and, if needed, actions were taken to manage heart failure conditions.
Results:
Fifty-four heart failures were detected for a follow-up of 12 months.
9 HeartLogic alerts were notified to the center and all of them required clinical actions:
- 4 diuretic dosage increase;
- 3 hospitalization for diuretic intravenous therapy;
- 1 cardioversion for AF (new onset);1 treated for Covid-19 infection and mild HF symptoms.
Three alerts occurred after diuretic therapy discontinuation.
The average time between HeartLogic alert and heart failure clinical event was 11 days (2-19).The mean HeartLogic value was 29±8, and the maximum value recorded was 43.
Conclusions:
- The HeartLogic algorithm is useful to detect HF worsening and undertake appropriate clinical actions.
- Telemedicine and device remote monitoring are very helpful tools allowing early detection of HF-related clinical conditions.
- This is of utmost importance in the era of CoViD-19 pandemic, when scheduled access to the hospital for routine follow-up appointments might be limited.

A 60 years old man with chronic coronary syndrome, diabetes mellitus type II, chronic kidney disease, hypertension and 30% of left ventricular ejection fraction, underwent a Resonate dual-chambers ICD implantation on February, 9th 2021, after an heart failure event. The Latitude remote monitoring system and HeartLogic algorithm were activated.
On March 29th , an HeartLogic alert has been notified to the center….