")

")
")


")
")



Acute cholecystitis
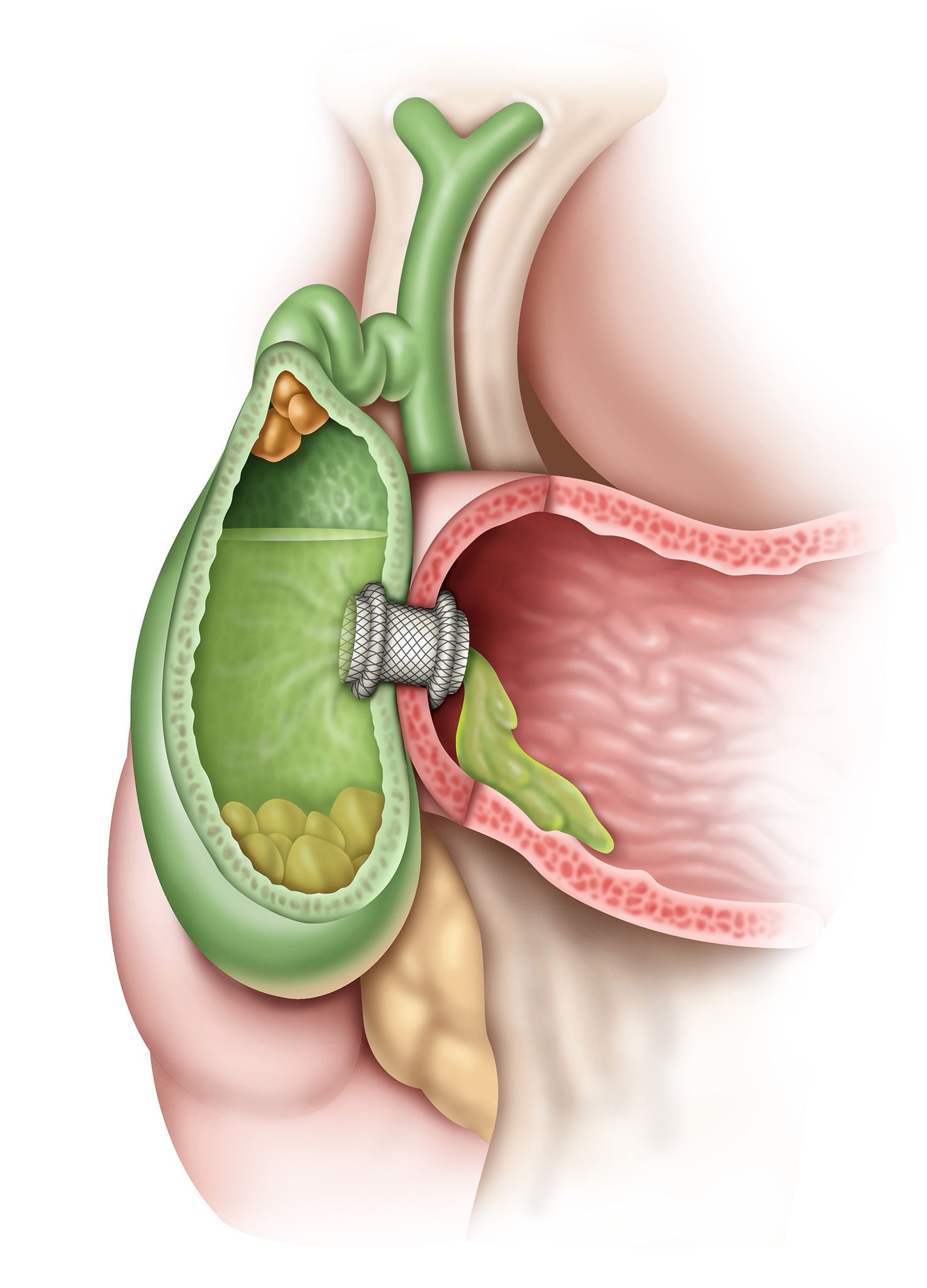
Acute cholecystitis is a complex disease often requiring urgent intervention. It is a gallbladder inflammation usually caused by a gallstone obstructing the cystic duct. Symptoms can include right upper quadrant pain, fever, nausea, chills and vomiting. Various approaches to its management have emerged, each influenced by advances in available technology, expertise of different medical specialists, and the unique needs of patients.
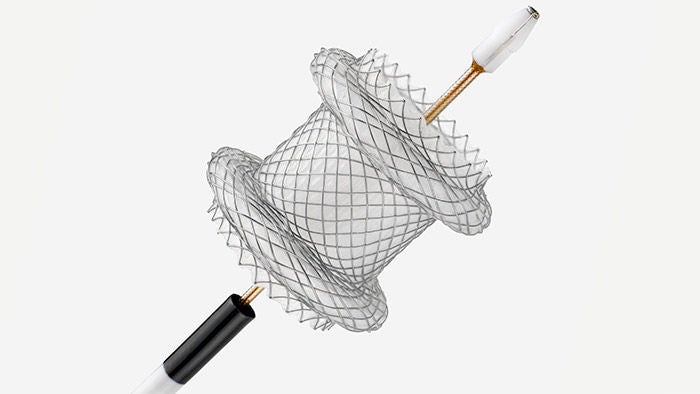
Hot AXIOS™ Indications
The Hot AXIOS™ Stent and Electrocautery-Enhanced Delivery System indicated for use to facilitate transgastric or transduodenal endoscopic drainage of:
- Gallbladder in patients with acute cholecystitis who are at high risk or unsuitable for surgery.
- A pancreatic pseudocyst or a walled-off necrosis with ≥ 70% fluid content.
- The bile duct after failed ERCP in patients with biliary obstruction due to a malignant stricture.
Acute Cholecystitis Solutions
Interventional endoscopy is a complex specialty, and we know its success relies on more than just therapeutic solutions. Read about our holistic gallbladder drainage solutions:
Enabling efficient and effective treatment procedures
Explore the treatment options for acute cholecystitis, clinical results, the roles of each specialist on a care team in optimizing patient pathway and their collaborative efforts in providing optimal care for patients.