







")

Interlock-18 and Onyx embolization endoleak type II
Baseline Central
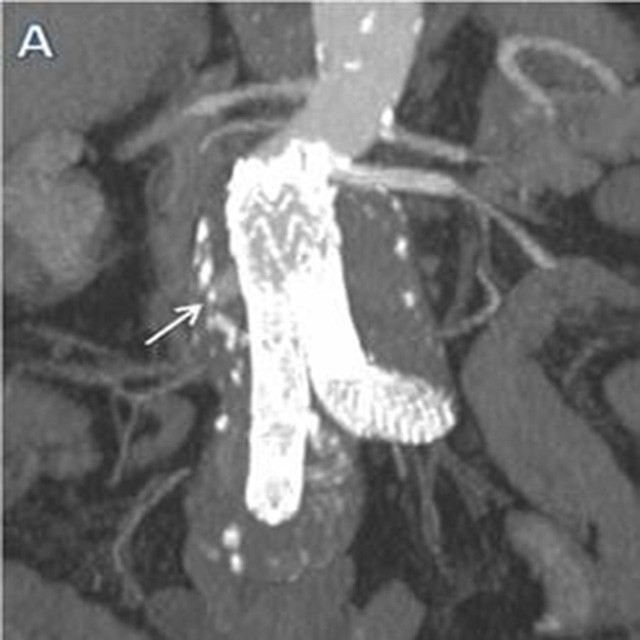
A 77 year-old male patient underwent left iliac branched Endovascular Aortic Repair (EVAR) with chimney technique for left renal artery, for an abdominal and left iliac artery aneurysm.
After 24 months with an MD-CT check-up a type II endoleak, of the inferior mesenteric artery, was diagnosed with enlargement of the abdominal aorta sac.

Trustable Pushability
With a 4F (1.33mm) catheter we were able to cannulate the middle colic artery.
We chose a Direxion™ straight tip 155 cm microcatheter and a Thruway™ guidewire. However the Thruway™ was too stiff to navigate in this tortuous anatomy.
We retracted the guidewire inside the microcatheter and continued without it.
Because of the pushability of the Direxion™ we were able to advance and cannulate the sac.

Embolization
The tip of the microcatheter was placed inside the “nidus” of the type II endoleak and was confirmed by sac angiogram.
We used a liquid embolic system to fill the sac and 3x120 mm Interlock detachable coil to perform embolization of the inferior mesenteric origin.
Despite a small perfusion through the coil, we waited a few minutes in order to allow the Dacron® fibers network to work because of its thrombogenicity.
Result
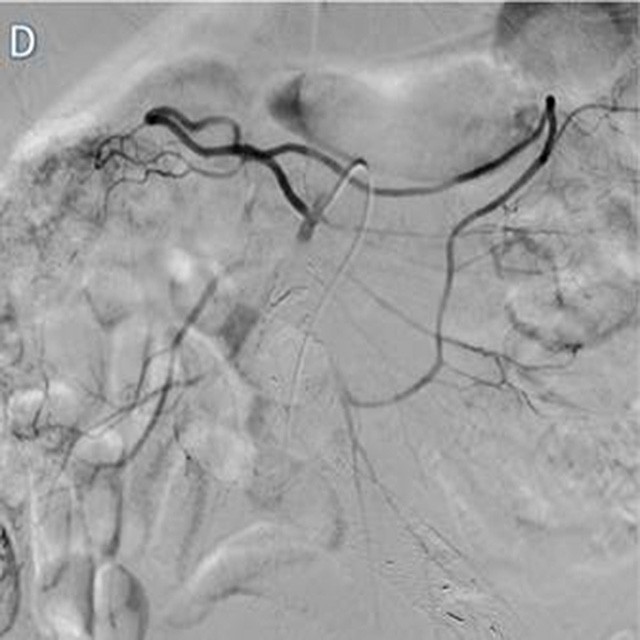
The final check demonstrated the complete exclusion of the previous type II endoleak, with perfect embolization of inferior mesenteric artery origin.
The patient was discharged on day two without complications. MD-CT and contrast enhanced ultrasound follow-up reveals no signs of endoleak with stability of the abdominal aorta sac.
Maurizio Cariati – Chief of Interventional Radiology Department – San Carlo Borromeo Hospital – Milano
Pierluca Torcia – Umberto G. Rossi (EBIR) – Paolo Rigamonti – Interventional Radiologists – San Carlo Borromeo Hospital – Milano