







")

An HCC Challenging Chemoembolization

Baseline Central
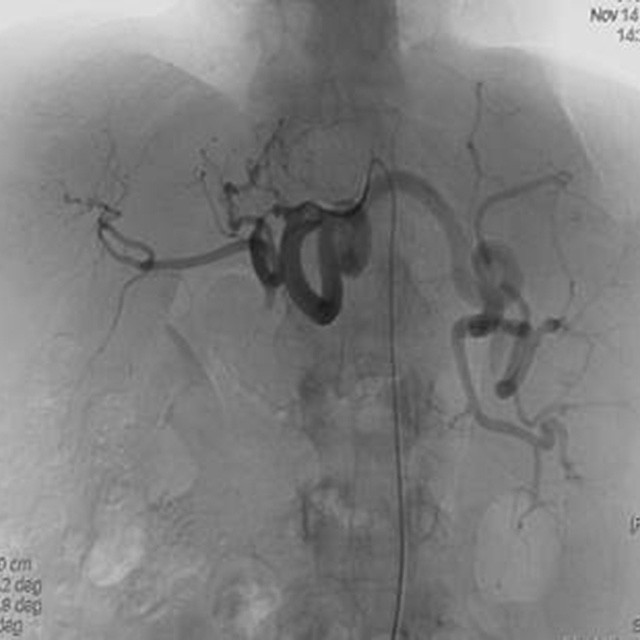
Diagnostic
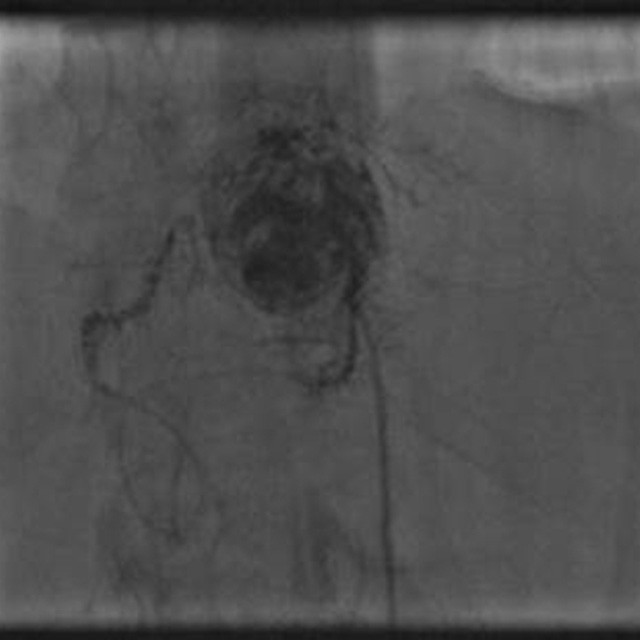
TACE
We decided to use an HI-FLO™ Direxion™ microcatheter 0.27" (0.69mm) and the Fathom™-16 micro-guidewire to overcome these anatomical difficulties in order to perform TACE more distally and more superselectively. So the stenosis was easily passed and we were able to catheterized the branch supplying the HCC nodule.
Treatment was performed by injecting 50mg of epirubicin mixed with 10ml of Lipiodol, followed by gelatine sponge
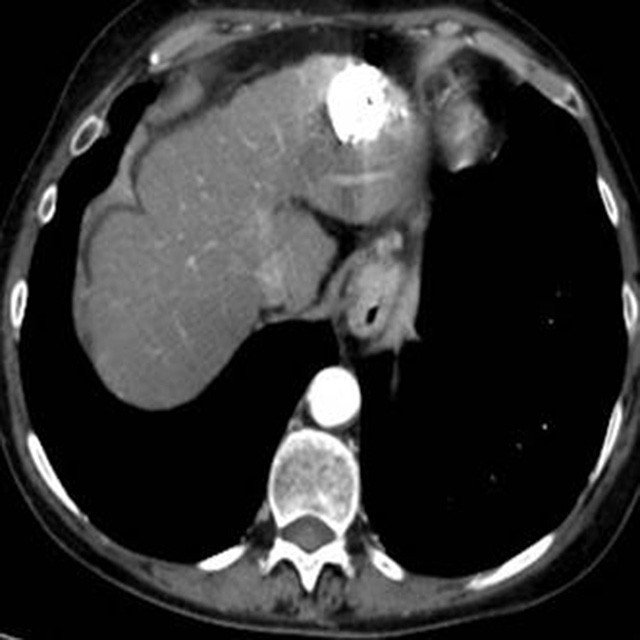
Result
The CT scan after the procedure confirmed the treatment of the nodule with a complete Lipiodol accumulation in the nodule and the absence of persistent disease.
The patient was scheduled to undergo a further TACE cycle in our institute for the remaining nodules.
Dr. Rita Golfieri – Chief of Radiology Unit and Vice Director of Department of Digestive Disease – Sant’Orsola Malpighi Hospital - Bologna
Dr. Francesco Modestino – Interventional Radiologist – Sant’Orsola Malpighi Hospital - Bologna