")

")

")
")


")
")



Lower Risk

Avoiding Complications with the S-ICD System
Transvenous lead complications are well-documented, and a major concern for patients1

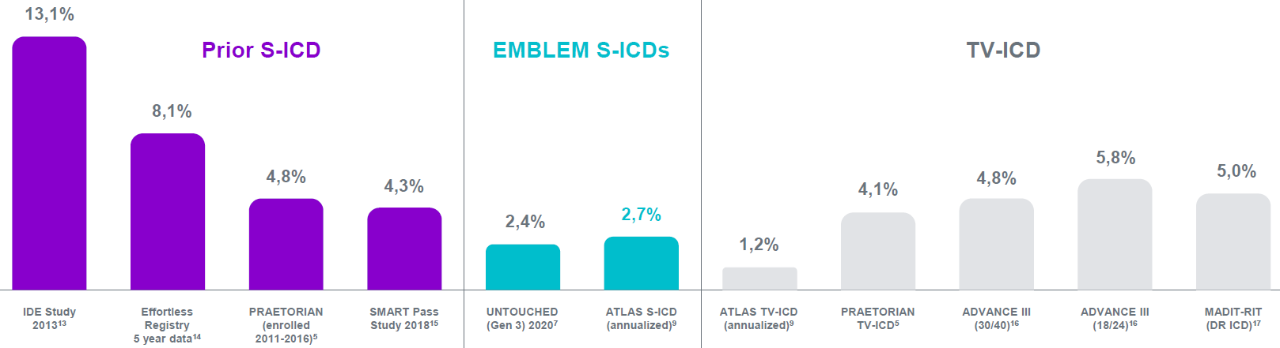
3-4% of patients with TV-ICD suffer lead malfunctions in the first year of implant10

About 25% mechanical failure rate for TV-ICD at 10 years10

4% infection rate for TV-ICD at 10 years10
The S-ICD avoids many of the complications associated with invasive leads, and reduces the risk of:
- Serious infections: secondary analysis of the PRAETORIAN trial showed patients with S-ICD had significantly fewer serious infections e.g. systemic infections, than those with TV-ICD2
- Avoids risks to vulnerable organs: extrathoracic placement avoids the major risks associated with invasive leads, while protecting patients from sudden cardiac death 3–9
- Complications associated with transvenous lead extraction (TLE): the transvenous lead is the most common source of complications in a TV-ICD system and transvenous lead extraction comes with procedural and post-procedural risks of complications1
This reduced risk was also demonstrated in the PRAETORIAN and ATLAS studies
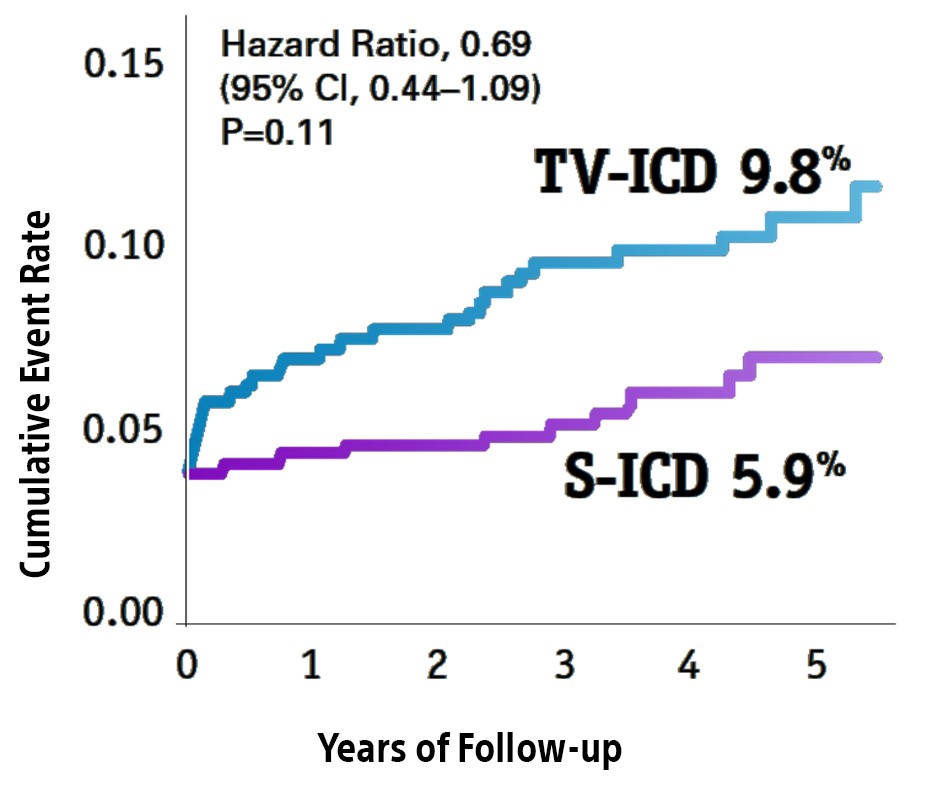
Over a median 4-year follow-up period, the head-to-head PRAETORIAN landmark trial*, demonstrated fewer device- and lead-related complications for S-ICD vs TV-ICD.5
Lead-related complications were significantly lower in the S-ICD arm.5
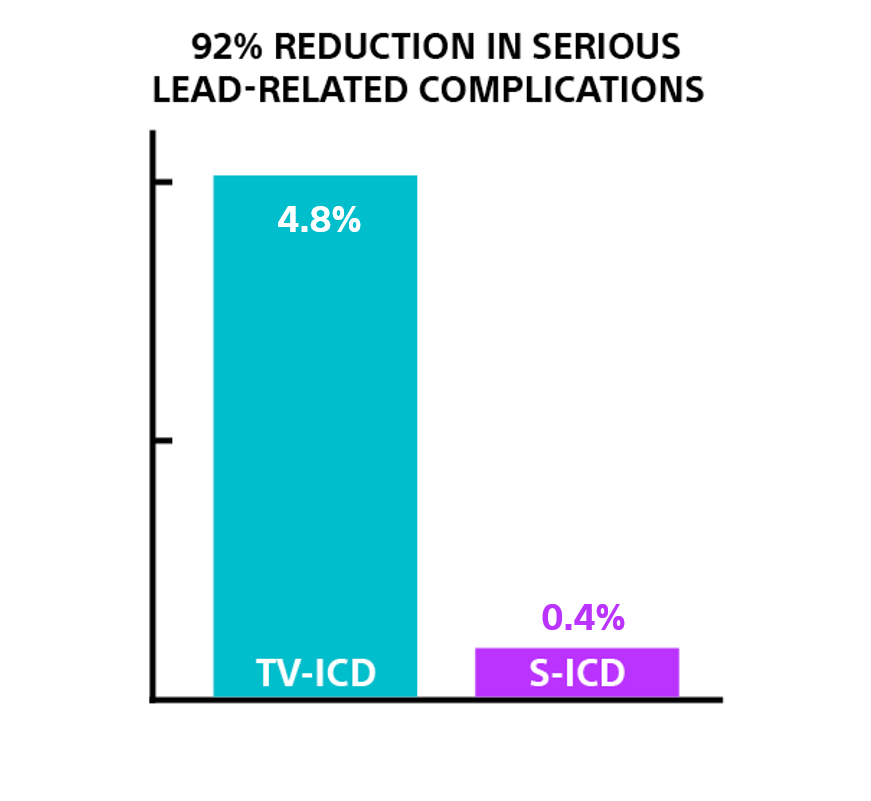
In the ATLAS trial**, S-ICD demonstrated a significant 92% reduction, in serious lead-related complications, at 6-months, for the EMBLEM™ S-ICD compared to any manufacturer's single chamaber TV-ICD (p=0.003).9

Data from a secondary analysis of the ATLAS trial‡ evaluated in nearly 450 patients the severity of Tricuspid Regurgitation (TR) at six months following the implantation of TV-ICD versus S-ICD. At six months, patients in the TV-ICD group were seven times more likely to have worsening tricuspid regurgitation (p<0.001) than those in the S-ICD group.
Appropriate therapy: S-ICD has been shown to have similar rates, aligned with TV-ICD.
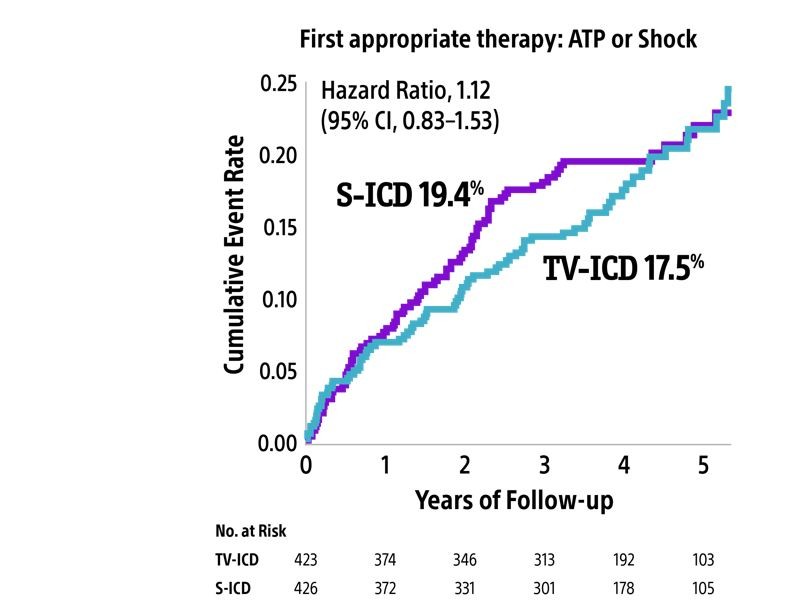
In the PRAETORIAN trial, appropriate ICD therapy was defined as ATP or shock therapy for either VT or ventricular fibrillation.
There was no significant difference in the number of patients with appropriate therapy (shocks or ATP) between S-ICD and TV-ICD (P = 0.45).10
S-ICD demonstrates low IAS rates