


")

")
")


")
")



Biliary Stricture Case: Elsa

Discover a patient’s journey, from diagnosis to biliary stricture management, adapted from a real case study. Patient name and other identifiable details have been changed.
Start of symptoms & initial assessment
Elsa Ferez, 49, was admitted with jaundice, dark urine, and worsening epigastric pain over three weeks. Blood tests found that Elsa had elevated levels of bilirubin (12.6), transaminases, and alkaline phosphatase.
Following further investigation, a CT scan of the abdomen and pelvis revealed moderate dilation of intrahepatic biliary ducts and a distended common bile duct to 14 mm. The dilated common bile duct transitioned at the head of the pancreas. No masses were observed in the gallbladder, bile ducts, or pancreas, and cholangitis could not be ruled out.
The ultrasound showed a distended gallbladder with sludge and possibly a small (5 mm) polyp. Biliary ducts were dilated, and no pancreatic masses were identified, possibly due to bowel gas interference. The recommendation was to consider ERCP for further evaluation.
Elsa’s treatment
1. First endoscopic retrograde cholangiopancreatography (ERCP) procedure
Elsa underwent an ERCP procedure during which the Autotome™ RX Cannulating Sphincterotome was used to access the common bile duct. A normal papilla and dilated intrahepatic ducts were observed. Notably, a constricting 'apple-core-type' stricture was detected at the distal third of the common bile duct.
A sphincterotomy was performed, followed by cytology brushings with an RX cytology brush. To manage Elsa’s symptoms while waiting for a diagnosis, an Advanix™ 10Fr plastic biliary stent was placed.

Cytology analysis of common bile duct brushings, including both smears and cytospins, revealed no evidence of malignant cells. While benign groups of ductal epithelial cells were observed, there were occasional atypical groups. Therefore, the pathologist expressed uncertainty regarding the diagnosis and recommended additional diagnostic tests for further clarity.
2. Multidisciplinary team (MDT) discussion
Upon reviewing the ERCP results, Elsa's MDT assessed elevated CA 19-9 and liver enzymes. All agreed further investigations were needed and endoscopic ultrasound (EUS) and cholangioscopy were deliberated as potential avenues for exploration.
Given the initial ERCP findings suggested intrinsic (cholangiocarcinoma) rather than extrinsic malignancy (pancreatic carcinoma), the team decided to refer Elsa to a facility equipped with cholangioscopy capabilities, in order to directly visualise the lesion and facilitate targeted tissue biopsy, ensuring a more precise diagnosis.
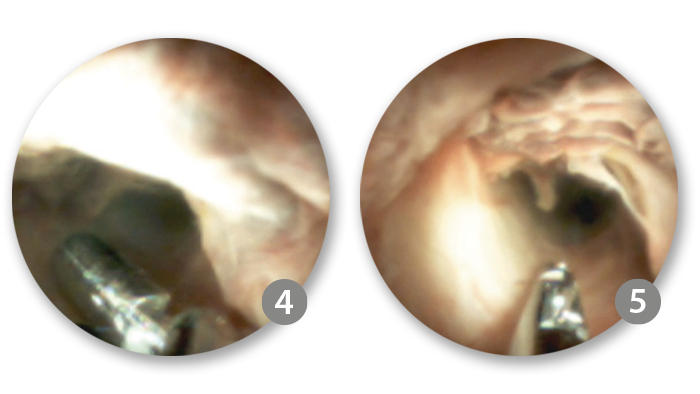
3. Cholangioscopy procedure
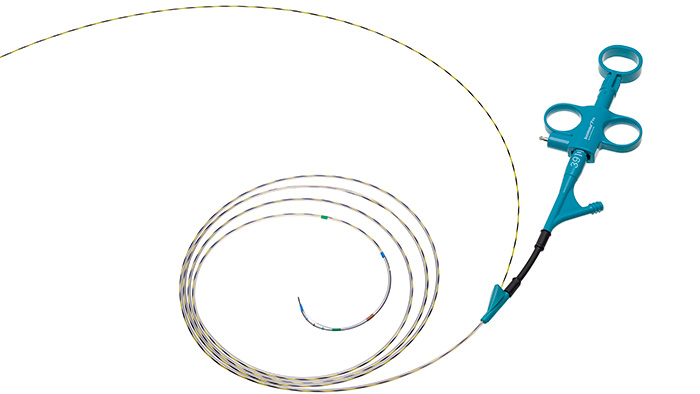
An ERCP with cholangioscopy using the SpyGlass™ DS System was conducted.
Following the removal of the plastic stent, the bile duct was re-cannulated using a Dreamtome™ RX. The initial cholangiogram reaffirmed the presence of a suspected malignant stricture, situated approximately 3-5 mm below the cystic duct take-off. Subsequently, the sphincterotomy was extended, and the SpyScope™ was meticulously inserted into the bile duct for direct visualisation.

The cholangioscopy with the SpyGlass™ DS System revealed normal left and right main hepatic ducts, along with the common hepatic duct.
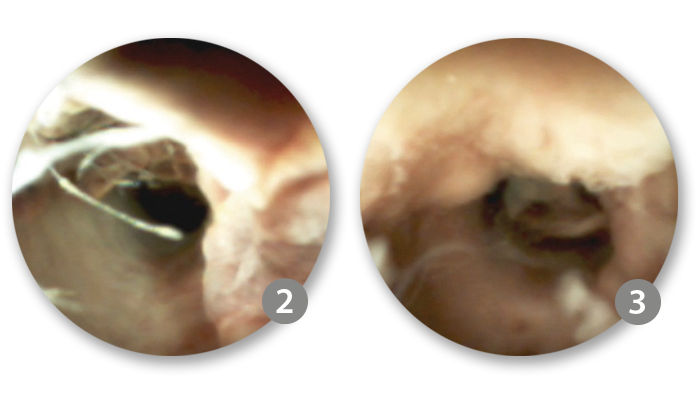
However, a mass lesion with atypical villiform growth and increased vascularity was observed in the proximal-to-mid common bile duct (CBD). This growth, occupying 50-100% of the lumen, exhibited characteristic features consistent with cholangiocarcinoma.
4. Targeted biopsy with SpyBite™ Max
The lesion extended from 3 mm below the cystic take-off, through the mid CBD and ended 4-5 mm above the ampullary insertion. Targeted biopsies of the biliary stricture were performed using SpyBite™ Max and frozen sections were prepared for pathology examination.

Watch a recorded procedure
Head to EDUCARE, our educational platform and watch a case of:
Early diagnosis of cholangiocarcinoma by SpyGlass™ Cholangioscopy
Or watch how radiofrequency ablation (RFA) could also be used to help manage biliary strictures:
Cholangioscopy-directed RFA of complex biliary cholangiocarcinoma
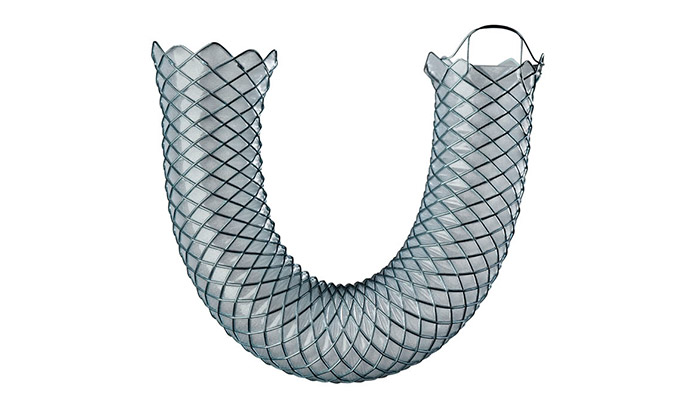
5. Biliary stricture management
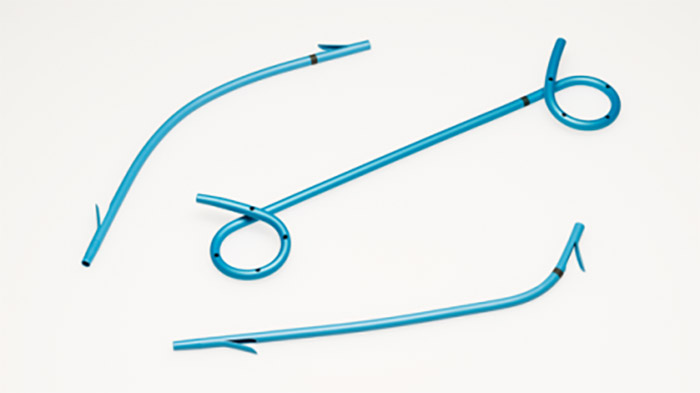
A WallFlex™ Biliary RX Fully Covered Stent System RMV (10 mm x 60 mm) was placed in the bile duct to alleviate biliary obstruction. This fully covered metal stent is approved to treat benign biliary strictures secondary to chronic pancreatitis, with indwell up to 12 months.*

6. Final diagnosis
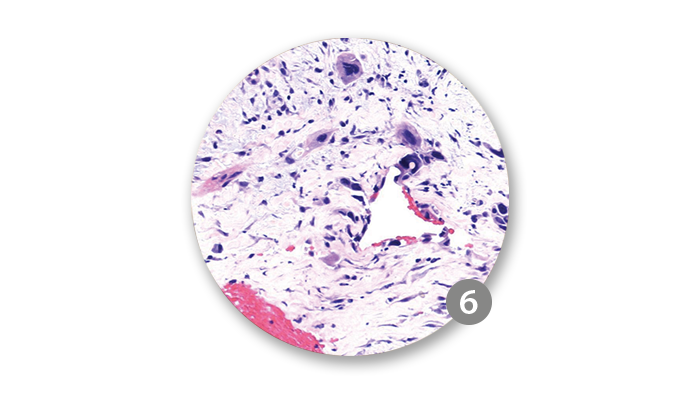
Intraoperative pathological examination of the frozen section revealed the presence of carcinoma. Subsequent analysis of all biopsies confirmed the diagnosis of cholangiocarcinoma. Elsa had to undergo an EUS and a PET scan to complete the staging process.
Removal of Elsa’s tumour

The patient's case was reviewed by the MDT, resulting in a consensus on T1N0M0 cholangiocarcinoma staging. Surgical oncology reviewed cholangioscopy, pathology, and ERCP findings, planning curative surgery for the well-defined mid-CBD mass. The patient underwent a successful Whipple procedure, including the planned removal of the fully covered stent during surgery.
The MDT's decision to proceed with the cholangioscopy-guided biopsy played a pivotal role. Without it, Elsa might not have been considered for surgery early enough, potentially compromising her long-term survival prospects. The use of the SpyGlass™ DS System may be able to accurately stratify patients for appropriate surgical intervention, thereby avoiding unnecessary procedures.