")

")

")
")


")
")



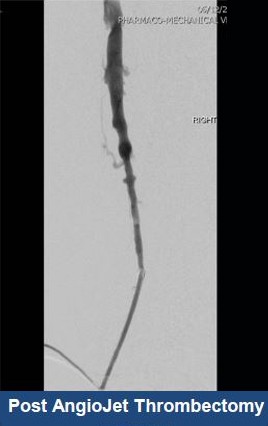
AngioJet™
Ultra Thrombectomy System
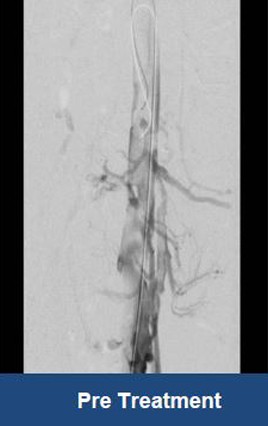
Thrombectomy of Massive DVT






Thrombectomy of Bilateral DVT




Thrombectomy of DVT

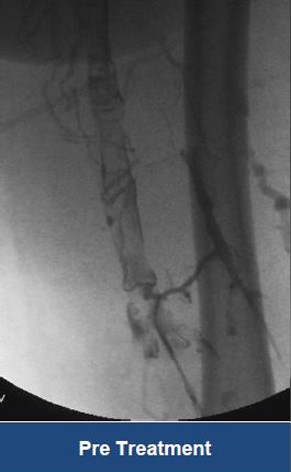
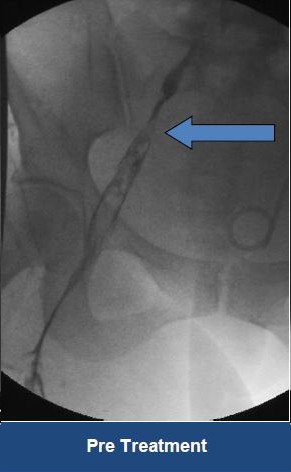
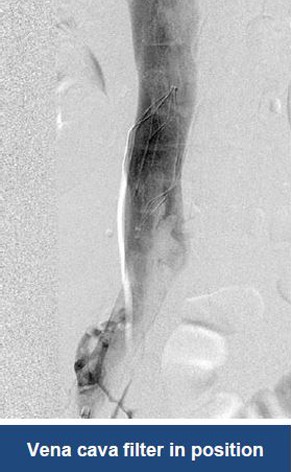
Treatment plan:
- Left popliteal access
- AngioJet Thrombectomy on affected areas
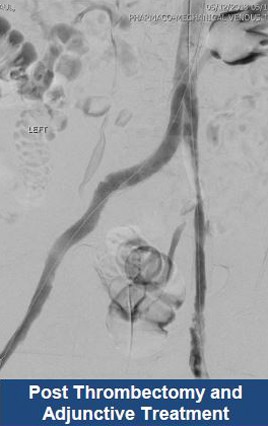
- Stent May Thurner lesion
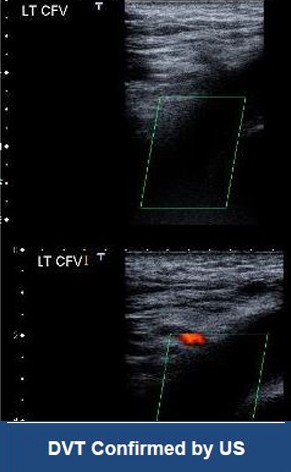





Thrombectomy of DVT
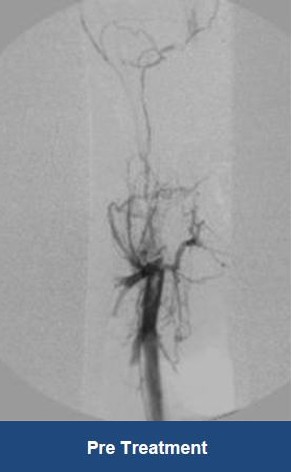

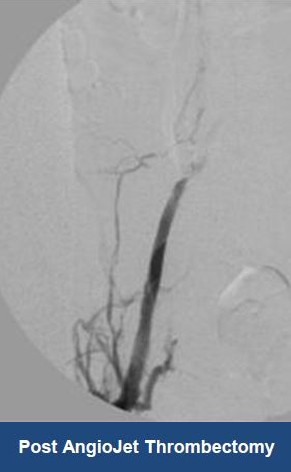

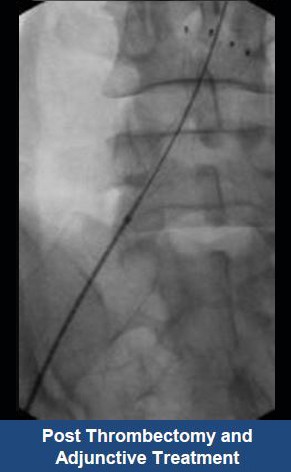

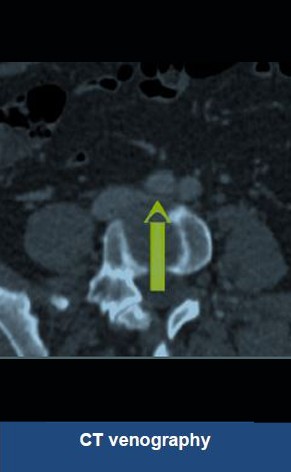
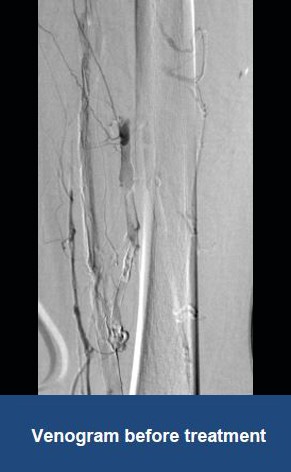
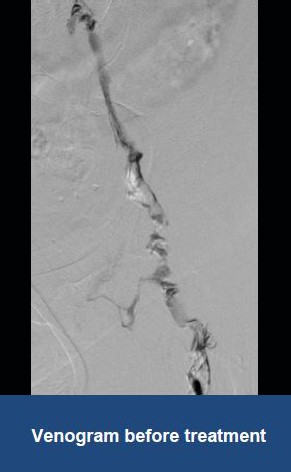

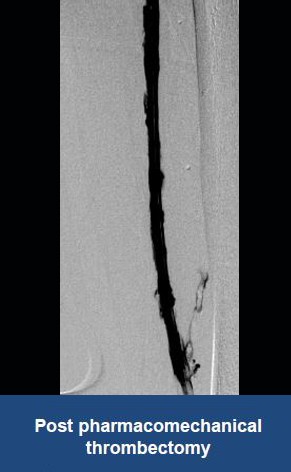

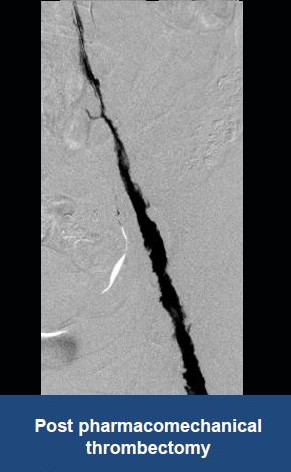
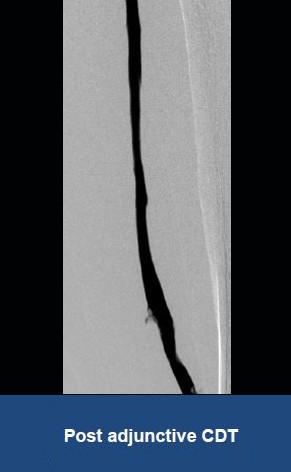

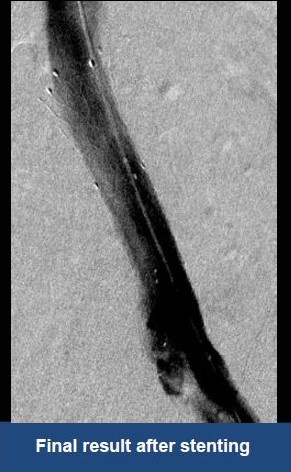
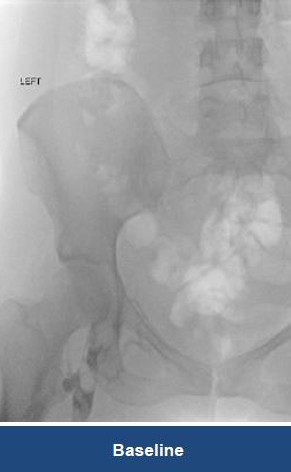
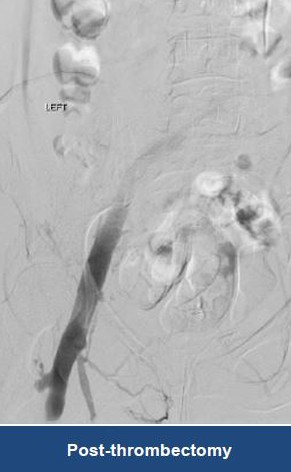
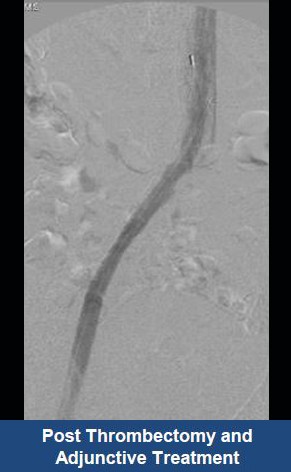
Thrombectomy of Massive Iliofemoral DVT and Stenting for May-Thurner Syndrome
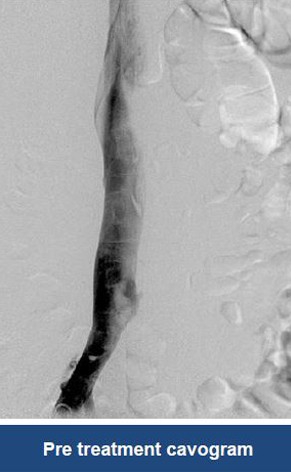


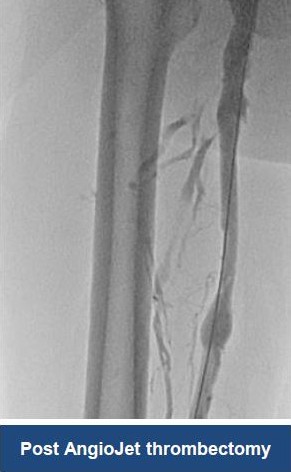
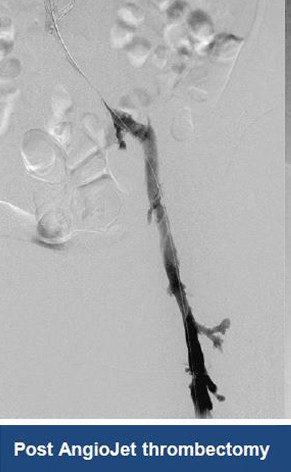

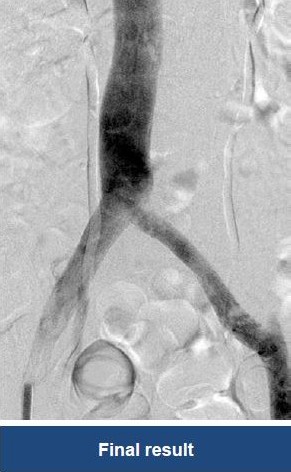
Acute Left leg Ilio femoral DVT managed with AngioJet™ Thrombectomy System and Wallstent Uni™ endoprothesis